CLINICAL DECISION SUPPORT
An outline of the use of decision support is discussed here. Since it is built into almost all of the clinical care processes, it would be discussed further in detail in the sections discussing each process. Care plans play an important role in clinical decision support and have been discussed separately.
Incorporation of Clinical Decision Support in CIS
Clinical care is a knowledge driven and information dependent activity. Modern clinical practice must be re-engineered to take advantage of the advancement in knowledge and practice of clinical sciences, management science, and information and communications technology. A Clinical Decision Support System that provides guidance and knowledge at the point of care is an integral part of the CIS.
Clinical decision support is envisaged not as a single system or application but as built-in functions within the whole patient care application (CIS) or its components. It is applied through several mechanisms:
- Guide to the data to be gathered and captured
- Guide to making a diagnosis
- Provision and matching of care plans for various categories of patients and at various phases of care
- Computer analysis and interpretation of results (normal, abnormal, scoring, stratification, grading, staging, comparison with standards for quality control)
- Provision of guides, instructions, alerts, prompts, reminders and suggestions
- Before or during the performance of certain procedures
- In response to certain situations, occurrences, incidents, non-conformance and abnormalities
- Provision of views of essential patient data according to needs at various instances of care (encounters) in the form of summarized just-in time and up-to-date data; especially for clinical support providers
- Selection, arrangement and presentation of the patient’s own data previously acquired or generated to help care providers make decisions (i.e. creation of views for specific purposes)
- Use of the hospital’s own analysed (aggregated) population data to guide decision making (e.g. selection of antibiotic based on incidence of bacterial resistance in facility)
- Provision of concise reference information, from either internal or external sources, on request or as a rule at certain identified steps in the care process (knowledge at point of care)
The clinical decision support application should be designed to match agreed policies, procedures and standards created and accepted by the hospital based on evidence-based medicine and best practices. It should also concur with the case-type or scenario based on interpretation of individual patient data and information derived from aggregated data of current patients with similar issues and problems (e.g. antibiotic sensitivity pattern, current disease incidence and prevalence etc).
Mandating Data Collection and Capture
Appropriate data collection and capture tools (forms) are provided to ensure that the care provider collect the essential data appropriate to the patient type (diagnosis) and phase of care (initial, tentative, definitive). This done by:
- Providing direction
- Providing choices
- Providing reminders
- Providing instructions and advice to the care provider
- Providing knowledge at the point of care
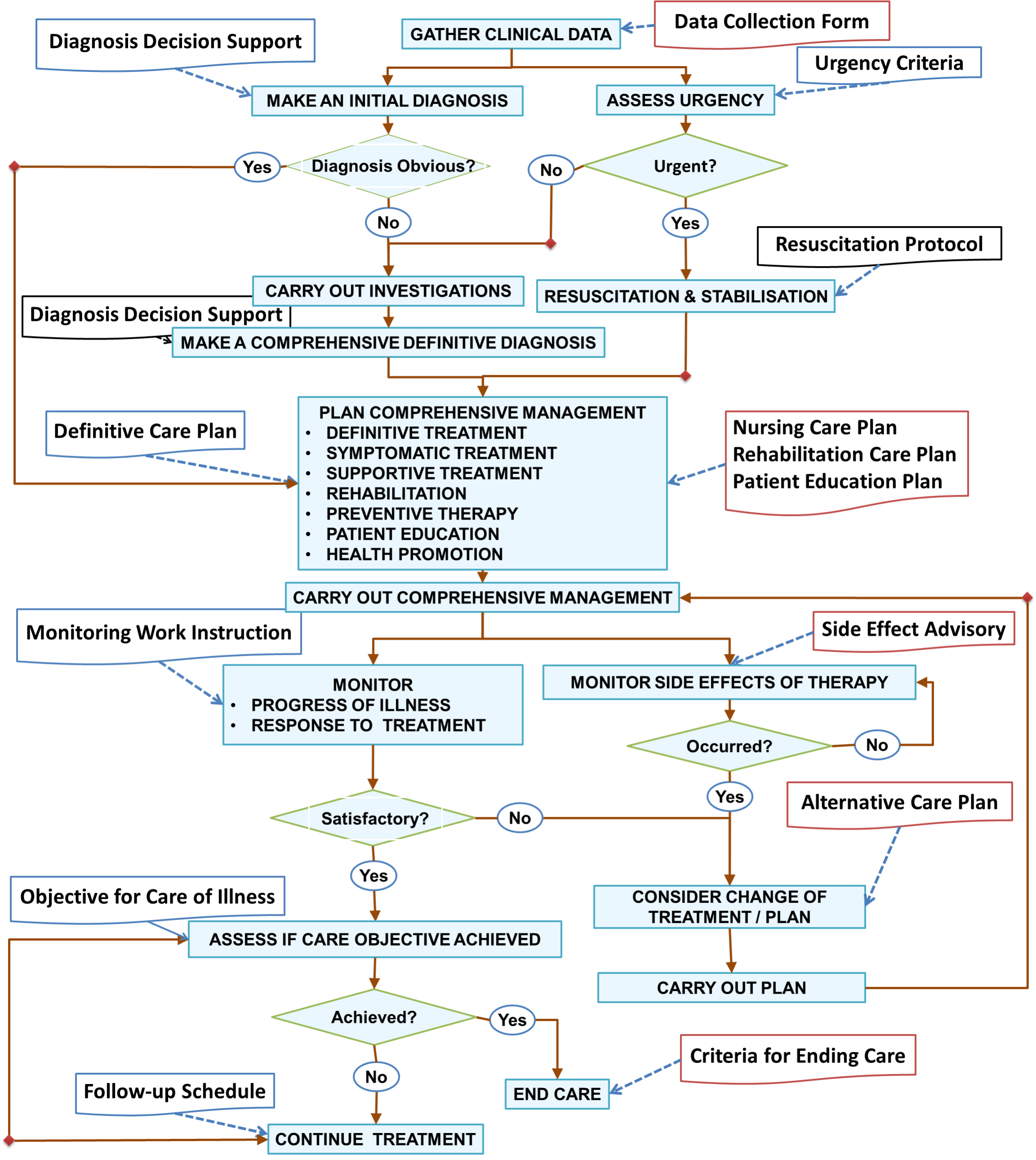
Providing Direction through Care plans
The whole CIS is designed such that the clinician is guided by care plans right from the first encounter based on the case type. He/she have the choice of adhering to the plan, to modify it or choose another care plan. There would be a change in direction if the diagnosis becomes more certain as more data is acquired and as the patient passes into a different phase of care; necessitating alteration in the choice of the next care plan. Hence, care plans are built for the phase when the diagnosis is at the level of symptom complex, clinical syndrome, disease class or specific illness. An important pointer to the direction is the reason for visit. Patients are identified as
- new cases,
- follow up cases
- cases of recurrence.
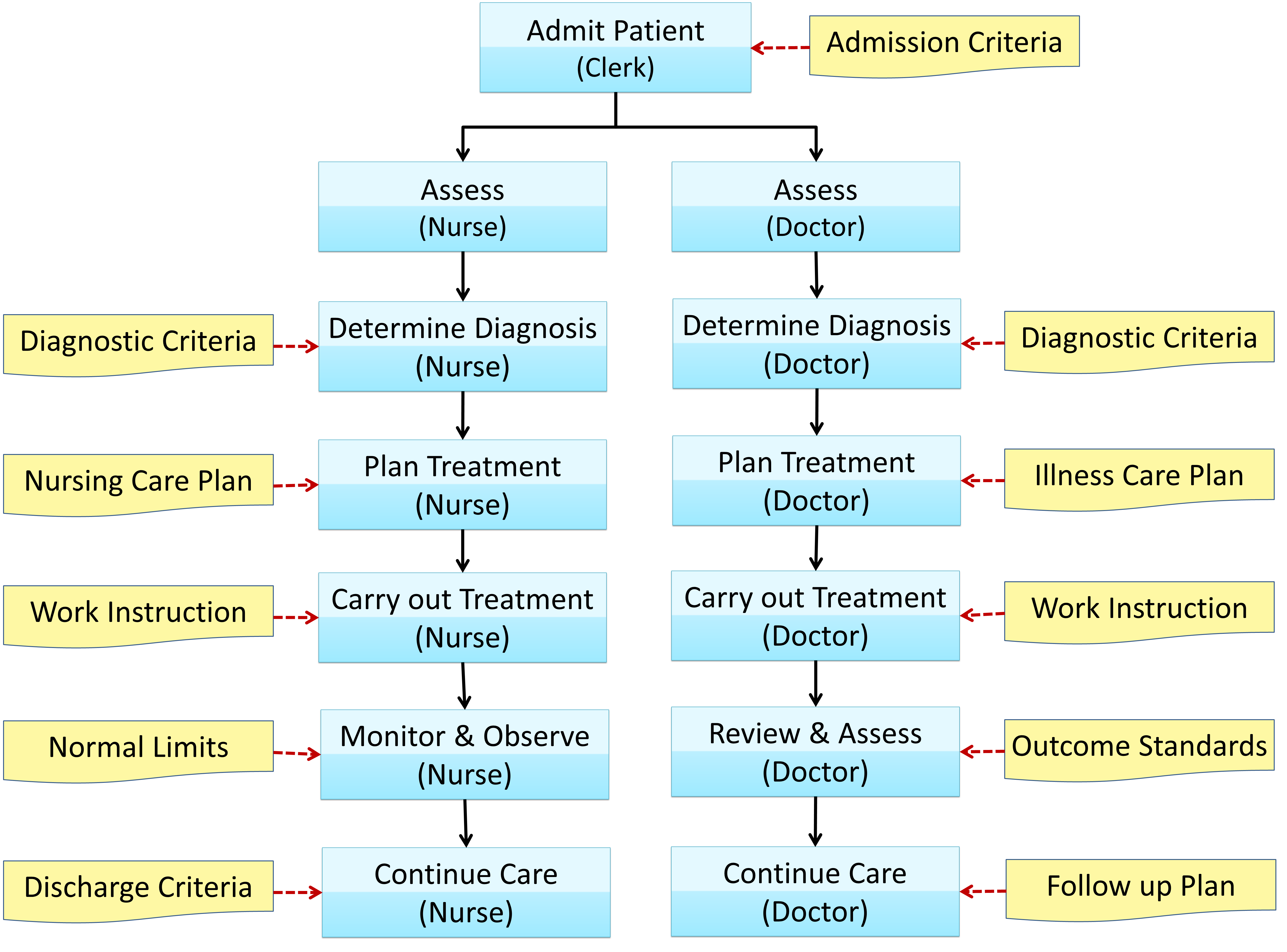
Subsequently, the main guide to plans would be the diagnosis and the phase of care i.e.
- initial (triage, resuscitation, stabilization)
- tentative (optimization of care regimen)
- definitive (continuation of definite care regimen)
Providing Reminders
There should be mechanisms to provide reminders on:
- Failure to complete or non-conformance to care plan
- Failure to act on an incident or variance
- Alerts may be given for instances when:
- An abnormal result or trend is obtained
- Shortfall in achieving desired outcome
- Presence or occurrence of allergies or untoward events
- Presence of underlying disease which may affect choice of treatment
A good method is to communicate these reminders and alerts through In Boxes (e-mail) within the system extendable to hand phones.
Providing Advice
The Decision Support System provides advice / suggestion / direction to the care provider regarding:
- Derivation of Conclusions (re: diagnosis, staging, prognosis)
- Further actions to be taken in the clinical care process such as alternative care plans
- Choice of modalities or methods to be used for:
- Investigations
- Monitoring
- Treatment
- Rehabilitation
- Continuation of care
Providing Work Instructions
While it may be assumed that being professionals, every clinician is familiar with various care processes; nonetheless some would welcome guides being made available. Some processes are so critical or so infrequently performed that the strict steps to be followed need to be provided didactically. Two alternative mechanisms available are to display the instruction as a rule (the push method) or to provide the means of requesting for it (the pull method).
It is expected that the Decision Support System should provide instructions on how to perform the following:
- Perform a clinical procedure
- Use a computer application
- Submit reports when an event occurs (Incident reporting)
- Submit data for registries and audits
- Provide mandatory reports to authorities e.g. notification of infectious disease
- Provide patient education
Diagnostic Criteria
A diagnosis is made by considering certain variables including signs, symptoms, clinical test results, investigation findings (laboratory, imaging, and endoscopy), monitoring parameters, clinical progress and response to treatment. Through research and experience the medical profession has identified sets of variables i.e. the criteria that predict a diagnosis. This knowledge can be presented to care providers to assist them in making a diagnosis. In certain instances, especially when a scoring system is used, these predictions have a high level of accuracy. For this purpose there must be a facility to assign values to each criterion, calculate the score and present it in a calculated data field. A comparison is made with the accepted scores to determine the likelihood of the diagnosis. However a rough guide can be just as useful to the clinician.
(http://www.isabelhealthcare.com/Scienceline.html)
Risk Stratification / Severity Grading / Staging
Having made the diagnosis the clinician needs to clarify further:
- which variant or grade of the illness is affecting the patient
- which stage of the natural history of the illness has been reached
- what complications has accompanied the disease
- how the patient has responded to the disease
This information allows the clinician to assign the patient into one or more categories according to disease variant, possible risks, severity of illness, stage of development and therefore prognosis. Categorization in turn allows the clinician to choose the right approach and initiate an appropriate management plan. Grading and scoring systems for various diseases have been developed and tested by healthcare professionals /specialty organisations. Their use depends mainly on applicability (e.g. are tests available in a timely and cost effective manner).
Indications and Contraindications for Use of a Method or Modality
Investigation and treatment modalities however efficacious has limitations such as unwanted effects like interactions, side effects, lack of effectiveness in certain situations (e.g. renal failure, hepatic dysfunction, cardio-respiratory impairment) etc. Care providers need to be reminded of these indications and contraindications as part of the decision making process.
Providing Knowledge at the Point of Care
With the availability of computerized information technology, an opportunity exists to provide relevant and accurate information as and when required (at the point of care). This information can be made available on demand (pull approach) or be presented automatically – activated by certain conditions or rules (push approach).
Types of Reference Information in Clinical Decision Support Documents
The information may come from two sources:
- Internal
- External
Internally sourced references include work procedure, work instructions and standards. Externally sourced references may include evidence based guidelines and basic medical knowledge such as anatomy, physiology, pharmacokinetics, staging systems, body mass index, surface area, nutritional requirements etc.
The Decision Support System can provide knowledge at the point of care regarding the following:
- Diagnostic criteria based on analysis of any or all of the following facts:
- symptoms and signs
- diagnostic test
- post-procedure finding
- Risk Stratification / Severity Grading / Staging
- Choice of various modalities for:
- Investigations of a clinical problem
- treatment (surgery, anaesthesia, invasive procedure, chemotherapy, radiotherapy)
- management of complications of a treatment regime (e.g. total parenteral nutrition, ventilatory support)
- Indications Contraindications and pre-requisites for use of a modality, drug or procedure
Provision of Knowledge at the Point of Care
PACKAGING OF INFORMATION IN A COMPUTERIZED SYSTEM
Implementing the concept of information at the “point of care” means that only pertinent information should be provided in relation to a work process. This necessitates the packaging of relevant information, be it actual patient data or reference information, in a precise, concise but adequate format. The user must not be inundated by “information overload” nor should the speed of delivery be impaired by sheer volume. Some data may be displayed as a mandatory view while others are hidden but available on request.
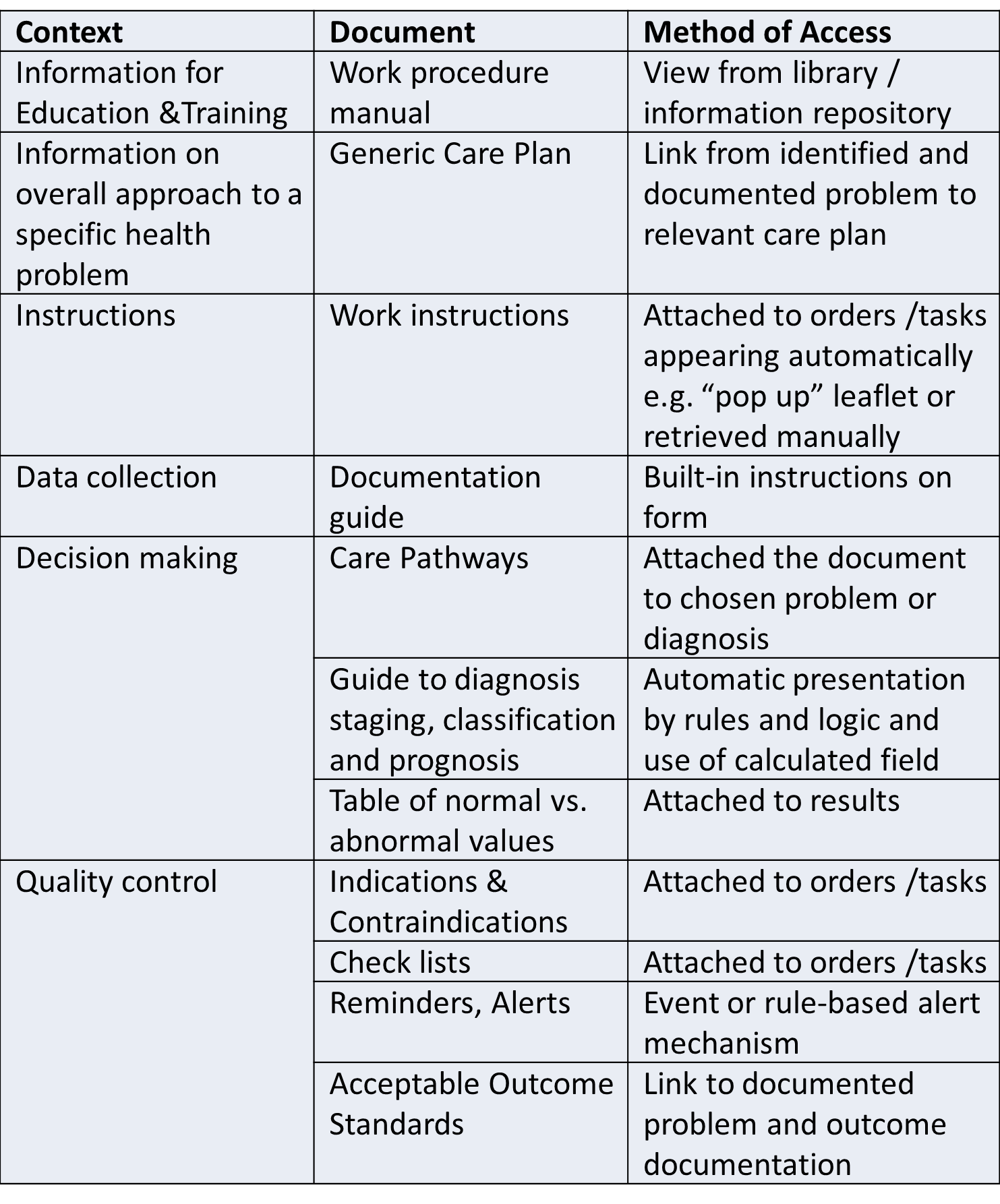
The amount of information required by a care provider depends on the stage of the care process and also the purpose for which the information is intended to be used. At the initial phase, the user may want to have an idea of the overall management of the problem. Therefore a summary of the entire management plan may be presented. When making decisions the care provider may require certain sets of criteria or scoring systems for guidance. At other times, before performing certain processes a work instruction or a reference table may be helpful. How these information packages may be provided is shown below:
Figure 4 10: Packaging of Information
Technical Aspects of Clinical Decision Support
There should be mechanisms to access reference documents for decision support. These include instructions for performing tasks using forms used for clerking, writing progress notes and order details. Therefore, the design of both types of documents needs to be streamlined.
The system takes full advantage of capabilities such as the electronic filing system and hyperlinks, to provide relevant and adequate ‘just-in-time’ information. For full implementation, a comprehensive set of reference documents that supports various functions at all levels of the clinical care process should be made available. A repository and retrieval system for reference information including a standard document identification (numbering, coding, URL) system should be maintained. Information required by a care provider performing a specific task can be made available at the relevant part of the documentation form. For example to retrieve a “Guide to Diagnosis”, a user can initiate a hyperlink placed adjacent to the diagnosis field in a clerking form. How this can be done is illustrated through the use of a work flow chart shown below:
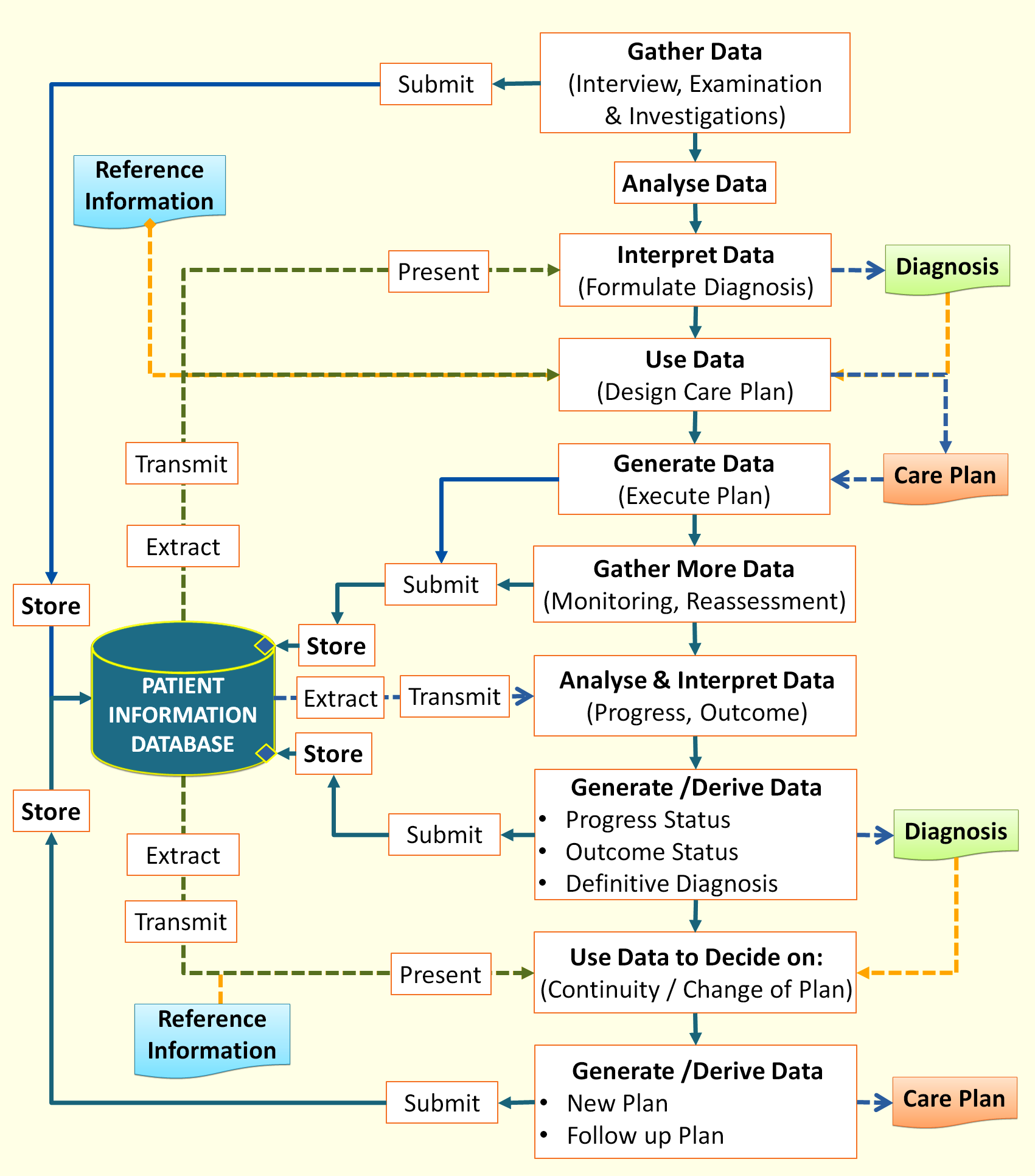
Conceptual Scheme of Clinical Decision Support System
Presentation of Care Plans and Decision Support tools
To use care plans, the clinical care provider selects the appropriate plan and corresponding order sets from a reference list. Once selected, these become processes or tasks to be performed. For clinical tasks, the process of documentation of results is mandatory and inherent in every task carried out. The forms or charts used can be attached to the tasks or selected in an ad hoc manner from a catalogue.
Care pathways, decision guides and quality control (QC) standards are provided as references either on request or is built-in and displayed each time a process is being carried out or an event has occurred. Suggestions should be limited to certain selected processes only to avoid clutter which can be annoying.
Content of Decision Support Documents
It must be noted that the decision support tools are part of the CIS and not necessarily part of the EMR. However, the plans selected should be recorded as part of the EMR.
Means of Providing Decision Support