
This description of the EMR is fundamentally different from what is perceived by most people. I believe that the means to create it as advocated here is already present in current computerized HIS, waiting only for the acceptance of the concept.
TRADITIONAL VS ELECTRONIC MEDICAL RECORD
The paper-based Medical Record consist of notes regarding the care of a patient written on sheets of paper arranged in chronological order and compiled into a folder. It is a log of events, the events being things done for the patient as well as things that happen unexpectedly. It does not provide all the means for the practice of patient care but serve several important functions. These functions can be summarized below:
- document and share information about a patient during the current patient care session or visit
- make available the completed record for use by subsequent clinical care providers to facilitate continuity of care
- maintain a permanent record for medico-legal and professional reasons
- make available data for the qualitative audit of an individual case (inquiries, case study etc.) and the aggregation of data from many cases for non-clinical uses such as research, audit, epidemiology and etc.
Use of the Medical Record Electronic or Otherwise
The Medical Record, electronic or otherwise, has the same function. The care provider uses the medical record for two main purposes:
- to be informed regarding the status of the patient and the care being provided
- to keep a permanent historical record of events that had happened during the care of the patient.
As a professional responsibility, all care providers are expected to record all plans, procedures performed, incidents that has happened as and when they are performed or happened.
From the legal standpoint, the institution where the care is given is responsible to maintain and make available a record of the care given and events that occur during the entire care episode.
Structure and Content of the Medical Record
The content of the entire medical record (be it paper-based or electronic) is predictable and defined. A major portion of the medical record is a record of events that are either planned or unplanned. Planned events are proactive clinical care processes or interventions. These include technical as well as cognitive (thinking) processes such as making decisions e.g. diagnosis, planning and interpretation of progress or outcome. Unplanned events can be incidents or developments that are part of the disease process or responses to interventions and actions taken. The event itself need to be described by accompanying facts such as:
- what happened,
- when,
- where and
- who are involved
- who makes the notation
Because of the need to be chronological, time elements (such as episode, visit, date, time by the clock) forms the basic framework of the EMR template. Encounter types, tasks performed and events that happen need to be named specifically and indicated as headings. Care providers involved and the person who documents need to be identified. The context within which the task is performed (e.g. indications) or events that happened (e.g. relationship to procedures or drugs) need to be clarified. As care processes follow an iterative (cyclical) pattern, headings in the EMR are also repeated until the care episode ends.
In principle, each medical record is a collection of information that:
- is a collection of data concerning a single patient
- contains information generated as the result of Clinical Patient Care
- is documented by health care professionals taking care of the patient
- the phrasing, words used remain true to the way they are recorded
- is arranged in chronological sequence (a log of events)
The Medical record contains the following groups of data:
- identification data and profile of the patient
- visit and encounter information (visit/encounter types, dates and time)
- information gathered regarding the patient’s illness and health status (symptoms, signs, test results)
- decisions and plans both immediate and long term (diagnosis, treatment plan)
- activities (procedures, tasks) performed for or on the patient (the time, the person performing it, the location, the method, the equipment used)
- events that occurred: planned (procedures) and unplanned (incidents))
- results or findings emanating from these activities and events (numerical, text or images)
- communications between care providers i.e. instructions, opinions, referrals and advice
Note: Reference for Content and Structure of Medical record can be reached here:
Characteristics of Paper Medical Record
A record is information that is retained. In a paper Medical record, information is written down using ink on paper. Once written, it is not supposed to be cancelled or erased. As such the data is said to be immutable. The only way the information is to be accessed is through reading the written record.
The paper medical record is a record of events (planned tasks as well as unexpected incidents). The record is made in a sequential (chronological) manner. Information about a new event is written as and when the event happens, in the space available after the previous event. In IT parlance, the information is said to belong to a time series data type. The date and time when the events happen, the type of event and who made the entry differentiates the events. Where the event happens is often not mentioned but assumed from the visit type. In some instances the record is made on printed forms (e.g. surgical operation notes), which are then retained and incorporated into the record. It is also common to record observations (Glasgow Coma Scale), monitoring parameters (Blood pressure and pulse) and results of tests (blood glucose level) on charts. Even though each item on the chart is in chronological order, the chart itself is often appended to the record at the end rather than within it.

Limitations of Paper Records
Care providers using the paper-based record are very dependent on having it at hand i.e. within reach. They try to ensure that information concerning the data gathered, the plan of care, what they intend to do, tasks done, the events that happen and findings/results associated with them are are written down. These notes are often called the case notes.
However, for many processes that they perform, the information is not captured in the Medical record for various reasons. For example, orders and prescriptions are written on the case note, but carrying them out require the use of extra short notes (forms, chits and slips) for placing orders or communicating between providers. The dispensing of drugs are often not recorded in the medical record because the record does not go to the pharmacy. Results are written or printed on result sheets which are pasted on to the record, often not in a chronological order vis-à-vis other processes. It is made chronological only when transcribed onto the right line or page of the case note, a practice that can lead to errors. Communications such as referrals are on letters or by phone such that their absence in the record make it seem that they were not done when reviewed later.
The medical record is also a communication tool. Indeed to ensure that care providers are aware of the status of the patient and what is planned for the patient, the medical record has to travel with the patient. Often observation charts, medication charts, result slips, x-ray films, the nursing notes or quite often, the entire record is not sent along (for various practical reasons), resulting in incomplete sharing of information between care providers. At the end of a visit, the charts and notes are compiled by care providers (usually nurses) before being dispatched to the medical record office where record officers will rearrange them according to a scheme.
In practice it is difficult to put together all pertinent information on paper to form an integrated record, even if serious efforts are made to accomplish it.
Difference between a Electronic Medical Record and Information Systems of Patient Care
It is important to differentiate between the Clinical information system (CIS) and the Medical record (EMR).
The CIS and the EMR are not Equivalents
The terms refer to two very different concepts and functions. CIS facilitates the work of patient care while the EMR is the means of recording data and making it available by displaying it, storing it as a document or printing it out.
The term ‘EMR System’ is inappropriate because it is not useful to have a computerized system just for retaining a record. Confounding the two terms lead to much confusion. It is not just a matter of semantics as some people are led to believe.
The CIS should not be considered or designed only as a system to generate the EMR. It has many more functionalities beyond the creation of a record. Instead, it deals with data that may not necessarily be considered as part of EMR (for example data used for communications, automation, quality control and administration).
The Electronic Medical Record (EMR), being a record of data generated as a result of clinical care processes (events, procedures or tasks) and incidents, is a product of the mix of data from the Clinical Information System (CIS) and the Clinical support systems.
In a computerized environment, most of the functions of the paper record (i.e. the capture, storage, distribution and communication of information) is taken over by information systems especially the Clinical Information System (CIS) with data also contributed by the various sub-systems of the Hospital Information System (HIS) . Because of this, it has the capability of incorporating data that is previously not captured in a paper based system.
Information through Use of Views Rather Than Records
While care is being delivered, the CIS provides information to the care provider as special views or displays pertaining to relevant aspects of the care via the graphical user interface. Although information is first entered via forms, it is not necessary to read from the form again. Instead, views are made to consist of data not necessarily from one form but can be a mix (aggregate) of data regarding the patient recorded by the same care provider or other care providers. A view is created for a particular purpose. For example the care provider can choose to see only the laboratory results as a spreadsheet or table view. Such views are actually reports i.e. information that is pulled from database tables appended with labels, headings, and graphics. The data can be sourced from any table within the patient information database and if necessary from other databases of HIS. The source of data can be from data fields within a single database table or from multiple tables. The queries are standard queries prepared in advance when the CIS is designed. Access to views are through links from menus and navigators.
Use Of Electronic Medical Record
The EMR of each patient, being extracted data derived from the operational database, is stored in a separate data repository primarily as a document with a defined content and structure. For most users it is mainly a read only document. Copies can be made available in a word processor document format, PDF or any other easily readable format. Being printable, hard copies of it can be shared.
Furthermore because the data is electronic, besides the narrative format, various types of data can be extracted, aggregated and presented as reports in the form of tables or graphs. These can be appended to the EMR. For example, a spreadsheet (table) view of laboratory data can be created and presented. It is also possible to select only a part of the laboratory test results and plotted against time e.g. Full blood count results over the entire episode of care. The same can be done for all results including nursing observations and Radiology reports.
The EMR is used during the active visit and subsequently as historical data. Therefore it has two main functions:
- A source of condensed information regarding the patient,
- during the visit,
- within the same care episode
- across episodes
- A comprehensive, relevant historical record of events for use as:
- evidence (in medico-legal and professional settings)
- reference information (research, statistics etc.)
The EMR as Views of Past (Historical) Information
Care providers use the Clinical Information System and other applications of HIS to plan and perform patient care activities. These software are used to plan tasks, create task lists and capture data generated by them, The system displays data to care providers as special views to aid them in organizing their work, look at relevant data and make decisions. The EMR is just another format for providing information, about what has transpired in the recent or remote past for the purpose of ensuring continuity of care.
While views are designed to display current information in real-time but because the EMR is compiled through various steps, the information may not be in real-time (historical).
Use of EMR during Care
It is important for the care provider to understand how the case develops. The EMR, as a chronology of events, satisfy this need. Therefore, a well developed HIS should be able to present data in the form of a Medical record both during care and afterwards as a historical record. A record should be created and made available for each event. As such, the current record is an accumulation of information about all events during each visit and finally for the whole care episode.
EMR as a Historical Record
Various legal and professional requirements (laws, regulations, statutes, rules and ethics) dictate that data of a single patient is presented as an accurate and complete chronological record (log) of events i.e. the Medical Record. As a historical record, it can then be relied on to show what actually transpired for the purpose of egal or professional inquiries. As such, the data must be accurate and complete. For this reason, when the HIS is designed, its ability to present the content and structure of an EMR must be seriously taken into consideration.
The Patient Information Database rather than the EMR is eminently more suitable for extraction and aggregation of data for statistics, research and quality management. An analytical database of replicated but anonymized patient data can be used for creating standard as well as ad hoc reports.
Use of Patient Information Database and EMR and Data Migration
As the Patient Information Database and the EMR contains pertinent data they also represents the essential mandatory clinical data that has to be retained and migrated if a new HIS is developed or acquired. Since the EMR is in the form of a document (in a word processor document format, XML or PDF ) the migration is much easier than migrating data from one database to another. Therefore, it is important to define what constitutes the pertinent information that must go into an EMR as required by healthcare professionals and as mandated by law.

Creating the EMR
The EMR is created by querying the patient information database. Each entry into the database is concerned with an event. Since all events consist of procedures, then each entry will have the procedure as the heading. The content and arrangement of the data in EMR are made to be consistent with the legal and professional requirements of a permanent record of all events and activities that happen during patient care.
The EMR being condensed in document format is more readable, easier to understand, and more amenable for use in inquiries and qualitative research. The format emphasizes the historical nature of the data. Quantitative data for research and other secondary uses should be obtained through queries of the database rather than from the EMR (will be discussed later).
- what happened,
- when,
- where
- who are involved
- who makes the notation
Constructing the EMR through Aggregation of Data
Derivation of EMR from Various Systems of HIS and the Database of Patient Data (Patient Information Database)
The Electronic Medical Record (EMR) is generated by extracting relevant data from the Patient Information Database which is an operational database where the data generated by CIS and other HIS applications are stored.
Sources of Data Making up the EMR
Unlike that of paper records, entries into the EMR are extracted from the database. The EMR derives data from multiple sources as depicted below:

Extracting Data from the Database to Create the EMR
The EMR is a document created and constituted through the extraction of relevant data captured through the CIS and other applications and stored in the Patient Information Database. A proper HIS should posses a built-in facility to present the EMR as an interim document continually updated at any time during the visit but more importantly, the completed record at the end of a session (visit). Because care providers are provided information through views, the it is not necessary for the EMR to be presented in real-time.
While the Clinical Information System (CIS) is seen as the system that facilitates direct patient care. The data generated by all clinical care activities are captured, and stored in the Patient Information Database is not the medical record until a defined portion of it is extracted and put together as the Electronic Medical Record (EMR). The EMR integrates and arranges in chronological order all the relevant information from various sources including those from Clinical Administration Services (described earlier) and Clinical Support Services (described in more detail in other articles on this website).

Records are kept for all events i.e. procedures performed as part of clinical care and unexpected incidents. The procedures include:
Maintaining the Chronology of Events
The EMR is a record of events experienced by patient during the course of care. The events can be made up of procedures performed or unexpected incidents as and when they happened i.e. in chronological order.
Incremental Updating of the EMR
The EMR is updated incrementally through the addition of new data (as in paper record) as an interim record rather than being extracted en masse from HIS at the end of a visit. There are instances when the availability of an interim EMR created from the data accumulated during the current visit is an advantage. It displays data in chronological narrative format for purposes such as overall case review by a person not familiar with the patient (e.g. doctor or any care provider to whom the patient is referred).
Data generated when different processes of care are done are kept in databases of various systems. It is necessary to create different applications and databases for different functions because each one of them follow unique polices and procedures. They generate different types of datasets. This means that data produced by the different systems for example laboratory results, images, drugs dispensed or administered, blood transfused and food plus beverage given can and must be included as part of the medical record. In the case of images only the pertinent ones need to be selected converted from the DICOM format into a format suitable to be part of documents (JPEG, PNG) before being included in the EMR.
Defining the Care Episode and Sessions
The care of a patient is divided into care episodes which is further into sessions with intervals in between.
- Care Episode
- Sessions
The EMR by definition is a record that is complete, continuous and sequential. It retains all information about the care of the patient for all instances. However, while providing care, it is important for care providers to indicate the service delivery instance in terms of:
- which care episode
- which particular session.
A session is primarily a visit which can be of various types.
- Care Episode 1
- Sessions
- Visit 1
- Visit 2
- Visit n
- Last visit
- Sessions
- Care Episode 2
A visit which contains events with each event made up of one or more procedures. An event can also be an incident.
- Care Episode
- Sessions
- Visit 1
- procedures planned in advance
- an incident and the procedures in response to it
- Visit 2
- Visit 1
- Sessions
Later when the full EMR has been constructed, care providers would have a complete picture of the patients problems, what interventions were done and the status of the patient. Administrators and researchers would be able to discern the various occasions when care is given, the team involved, the locations and so on.
Because the EMR is an extract of the Patient Information Database, a special query can be fashioned to produce a partial EMR concerning a particular care episode. For example, if the patient is being treated for the problem of “Cataract” an EMR containing data from the Cataract episode and sessions can be made available to the Ophthalmology unit. Summaries of the EMR can also be provided to other clinical units being consulted and clinical support units e.g. Pathologists, Pharmacist, Radiologists. Endoscopists, Dietitian, and Therapists.
RECORDING EVENTS
Events happen during sessions. For example the session can be the first visit. At the start the usual event is the initial consultation or clerking. This consists of a few procures namely: clinical data gathering, making an initial diagnosis and ordering some investigations. The time that the event happens (given a time stamp), what procedures were performed and the results (data collected, the diagnosis and orders made) are recorded in relevant database tables. To construct the EMR data is extracted from those tables and presented as a report.
- Visit registration, admission, transfer and discharge
- Information collection procedures
- Planning of care (Care plans and orders)
- Procedures diagnostic or therapeutic performed by a care provider at any service delivery facility including the emergency department, the outpatient or inpatient services,
- Laboratory test(s) on a specimen obtained from him/her even if not attending any of the other clinical services
- Imaging examination(s) performed on any part of his body even if this is the only service given to the patient.
- Dispensing of any drug from the hospital’s pharmacy service even if not consequent to a consultation (e.g. encounter to collect repeat medication)
- Transfusion of blood products
- Communications between care providers (referrals, consultations)
- Review of information and deriving conclusions or opinions
- Reporting of incidents and responses to them.
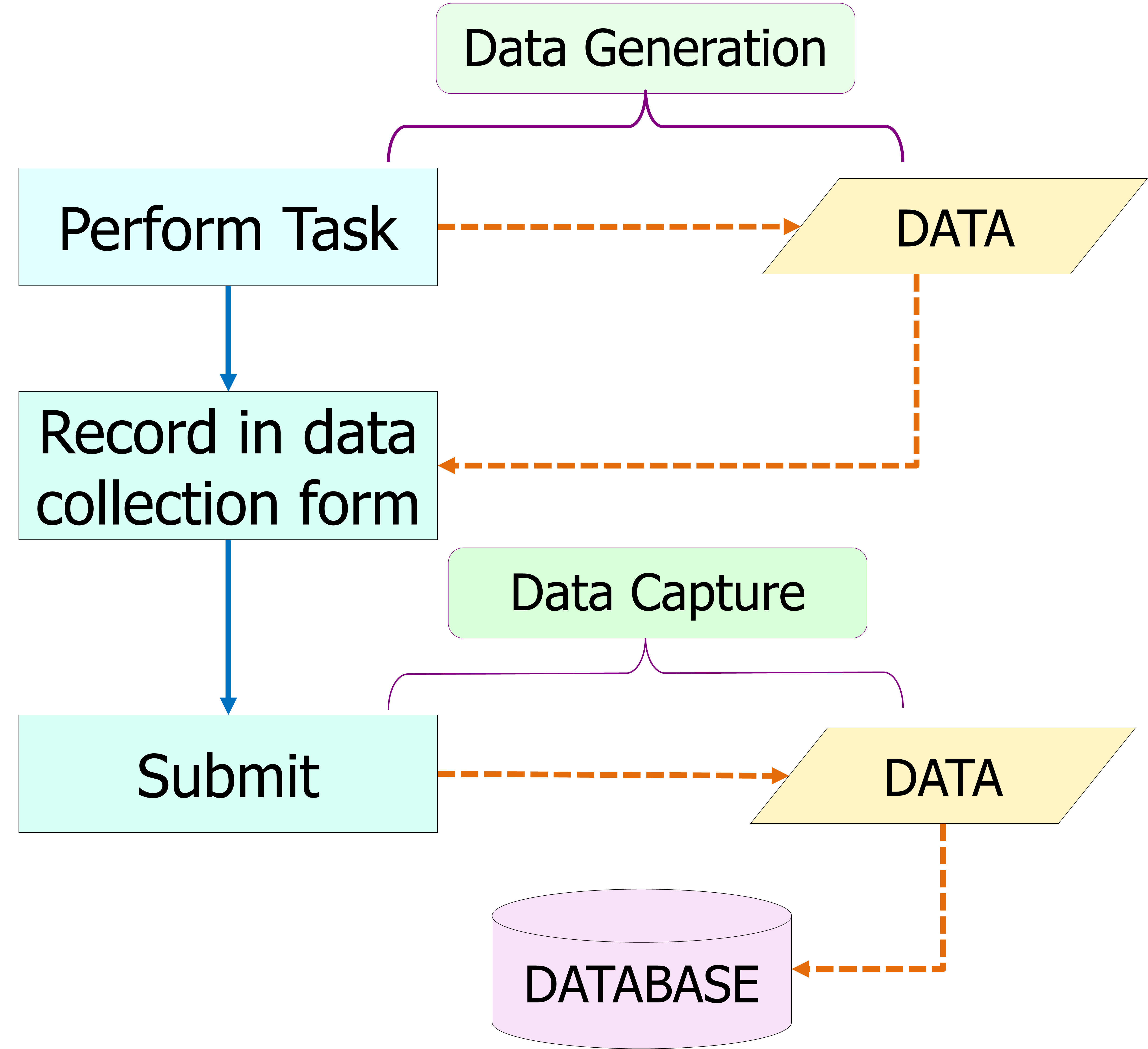
Data Collection
In paper records the data collected is mostly unstructured. Information is recorded as text sometimes with headings to differentiate sections. There instances in certain facilities where instead of plain paper printed forms are used and data is inserted into data fields. On the other hand the in the CIS, as far as possible the data collected is structured to enable data to be stored in databases and be analyzed. Data is placed in specific data fields such that the value for each field is restricted to predetermined data types and constrained values.

Data Storage
Data collected via the forms are distributed to various database tables. Each data field on the form is a representation of a data field in a database table.
Presenting Patient Data as Views in the CIS
Transforming Patient Data from Forms to the EMR
The structure and content is not unlike paper medical records and follows specifications of the medical record agreed by authorities (e.g. the Ministry of Health or Medical Council) or mandated by law. However, unlike in paper records, the instruments used to collect data such as forms or questionnaires do not become part of the EMR. They are only the means of obtaining data. Whether the data truthfully represents what the care provider has documented will have to depend on data integrity mechanisms built into the database. Exception is made for certain legal documents such as consent and notification forms which may be made available in the format prescribed by regulations.

Methods must be found to display data acquired during the course of clinical care in chronological order to reflect the EMR as a log of events.
Using Forms to Record Clinical Data
Transformation of Data from Forms in CIS to Text in EMR
In the end, the presentation of data in the EMR will be quite similar to that in the paper record.
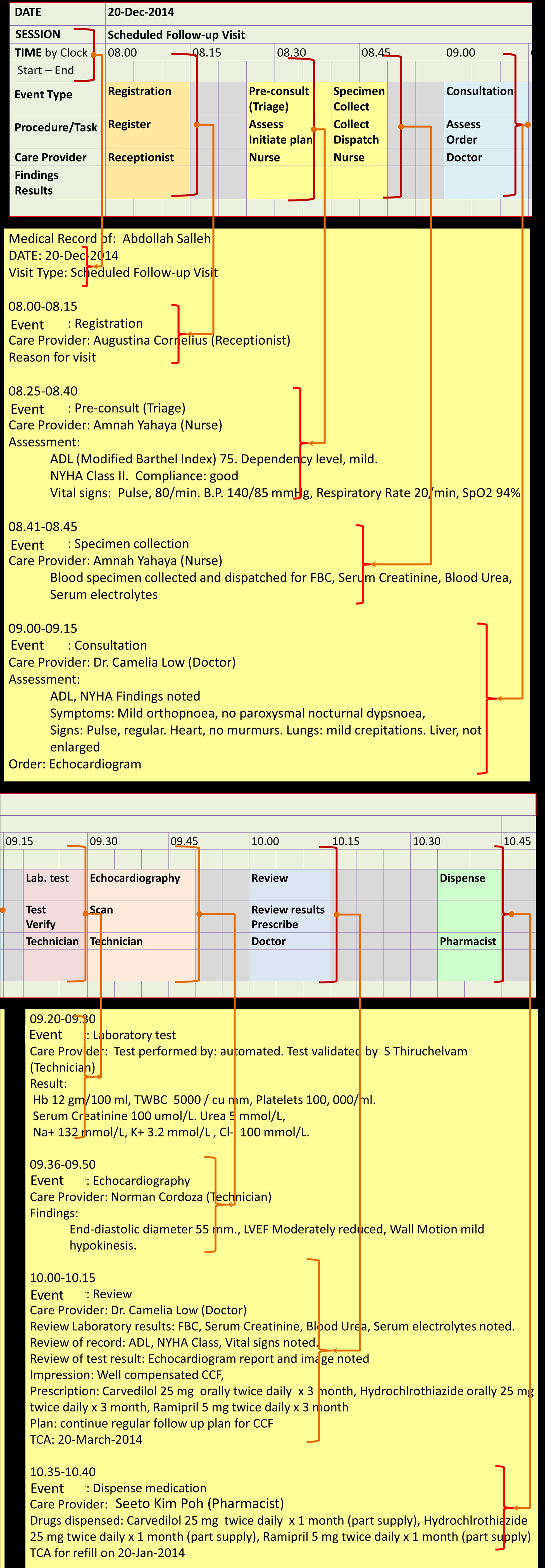
Presenting Clinical Data in Chronological Order
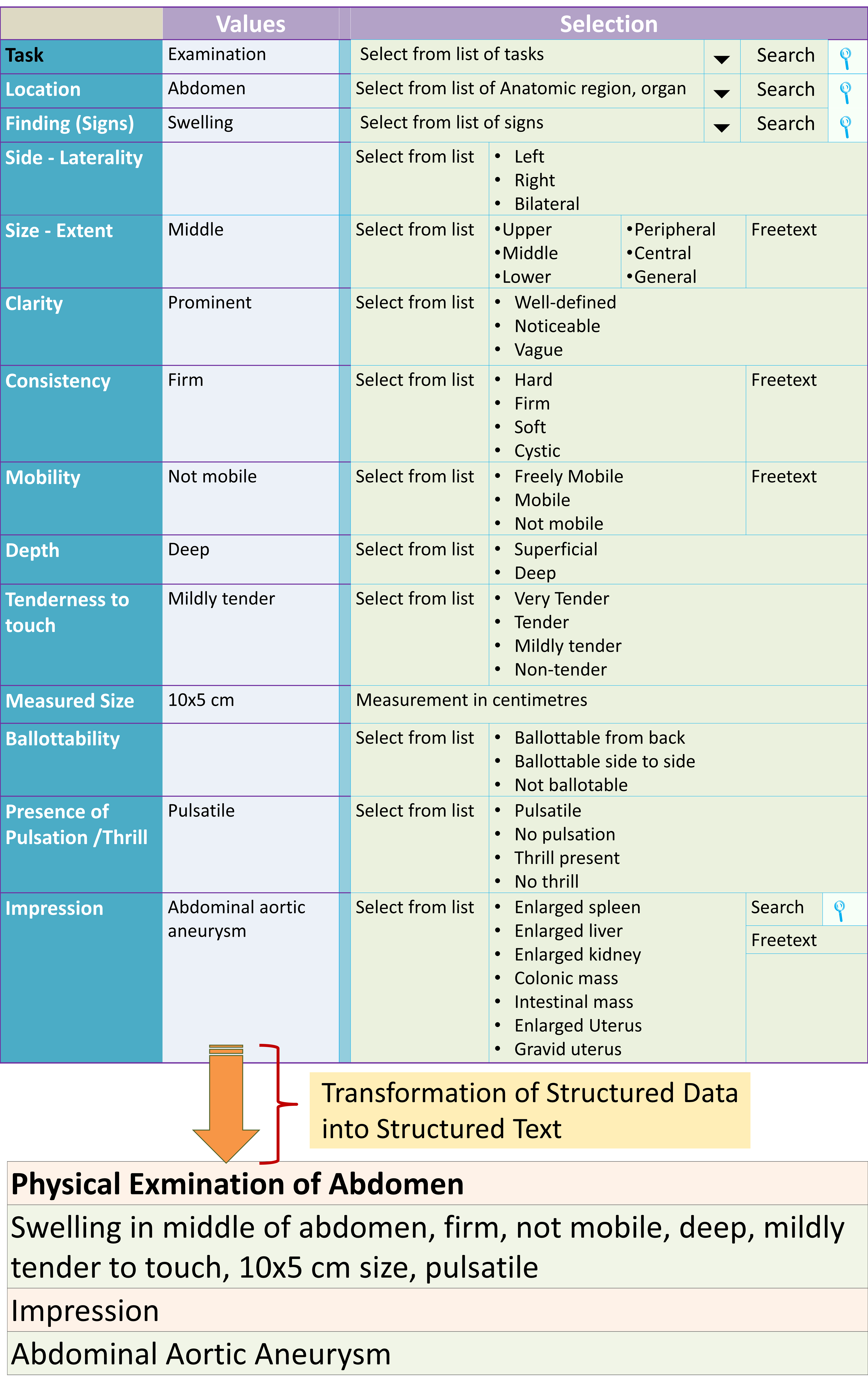
Conversion of Structured Data Into Text
While data in the CIS is necessarily structured, data in a medical record is better understood in text format. However. as opposed to paper records which are written freehand, as it were, the electronic medical record would be created by converting structured data into a text format i.e. it should use all the capabilities of structured text. It is important that the words and phrasing used by the care provider who documents the data is retained. The main method of converting structured data to text is through concatenation i.e. combining the values of multiple data fields into one. For the purpose conversion to structured text, fillers and interpolations such as conjunctions may be used. Rules regarding their use need to be spelled out and agreed by the clinicians.
The ability to convert the structured data of the database to text (narrative) format must be an essential function a proper CIS or HIS. The main way is to aggregate data through the process of concatenations. This is a process that requires some expertise.
Derivation of EMR from Various Systems of HIS and the Database of Patient Data (Patient Information Database)
A good example of the use of concatenation is in expressing diagnosis. Diagnosis consist of many data elements. The method used is discussed in the article below:
Integrity of the Record
A medical record must be matched to the correct patient. To ensure that each patient has only one medical record, the system enables the person performing registration to search for an existing record by the medical record number if it is available or otherwise any other unique identifier such as national registration number or name.
The entire medical record is an aggregation of records of individual visits, each visit being defined by the period between the registration and discharge or check-out. Each visit should be given a unique identifier (the visit number) which may be also used as the financial number.
Notwithstanding the above, means are provided for providers to enter or modify data for a short defined extended period after the visit ends. This allows for incomplete records to be updated if necessary. Care providers providing care during the visit are responsible for ensuring that medical record entries are accurate and complete.
There is also a mechanism for care providers to make notes outside of visits (reminders, communications, “sticky notes” etc.). These may be considered as part of the EMR if they relate to actions relating to patient care e.g. advice or communications given via phone or e-mail.
STRUCTURE OF THE MEDICAL RECORD
HIS applications and the database are designed primarily to support the operations of each of the services. The data required to be collected, presented and used are detailed. Only some pertinent data from each sub-system need to be sent to the Patient information database and subsequently presented as the EMR.
The structure of the EMR is different from the CIS in certain parts but is similar in many parts. As a historical record, the whole EMR should be arranged in a strictly chronological order regardless of the data source (discussed further later).
The same identification data from Patient Management System is used throughout the EMR.
Data obtained from other care providers from outside of the hospital are indicated as such. They are uploaded from portable storage media (flash dives, thumb drives, portable hard disks and CD-ROMS) or directly via interfaces with central regional/national data repository. Data in hard copy is converted to scanned images and appended to the EMR (rather than transcribed).
The main source of EMR data is from the CIS ,where data is actively documented as part of the clinical processes (clinical documentation). The clinical support systems are the other major sources where results destined for the EMR is automatically transferred. Results produced by clinical support systems (laboratory test results, imaging reports, supplies by Blood bank, Pharmacy and Dietary unit) are inserted in the chronology of events at the time they are performed and when results are available.
Radiology images are considered as part of the EMR. If they are stored separately there should be mechanisms to indicate their existence and relationship to the events recorded within the EMR. They should be retrievable as and when required.
Functionality for Incorporation of Paper Records as Part of EMR
The CIS application should also allow various hard-copy documents such as referral letters, printed results, and summaries whether produced by the hospital or supplied by other health care institutions to be scanned using a document scanner and stored in a standard image format(s) and kept in the Patient Information database or a repository linked it.
The system should have in-built mechanisms for ensuring that images are matched with the patients that they belong to.
Such images should be made available as part of the EMR.
Chronological Structure of EMR
The EMR being a log of events is chronological. Some data may be divided into temporal segments with each segment representing a visit or the intervening period. There are differences between outpatient and inpatient visits; mainly in terms of duration of visit and number of events per visit. Periods of visits are defined by date and times of registration (arrival) and discharge. During visits, activities consisting of planned or unplanned events are carried out at events which can take the form of interactions between the patient and various care providers termed as encounters. Events not requiring face to face interactions (non-encounter events e.g tests performed by machines) are also carried out. During each event any number of tasks are performed. Events can also be unexpected happenings (incidents) that occur during the visit.
Traditionally, the EMR may describe events within a disease episode or a care episode within one health care organization. However, it can also be merged with the EMR of another health care facility and health promotion and disease prevention activities, in which case it may considered to as a life-time health record or a vertically integrated medical record (often mistakenly called Electronic Health Record or EHR).
Content and Arrangement of EMR for Each Visit
The challenge of arranging patient data as a chronologically sequenced record can be resolved by considering the record as a diary or log. Each entry refers to an event and the data relates to various care processes (tasks) and incidents. The structure mimics that of paper records.
Just as in paper records, the main body is a log of the clinical care processes performed or events that happened as documented by clinicians. All findings and descriptions of care processes and events for this section must be chronologically sequenced and contiguous i.e. there should not be gaps in between. It includes:
- Administrative processes (admission, transfer, discharge)
- Assessment
- Progress Notes
- Diagnosis
- Plans
- Treatment given (medical, procedural, psychological etc.)
- Monitoring
- Outcome
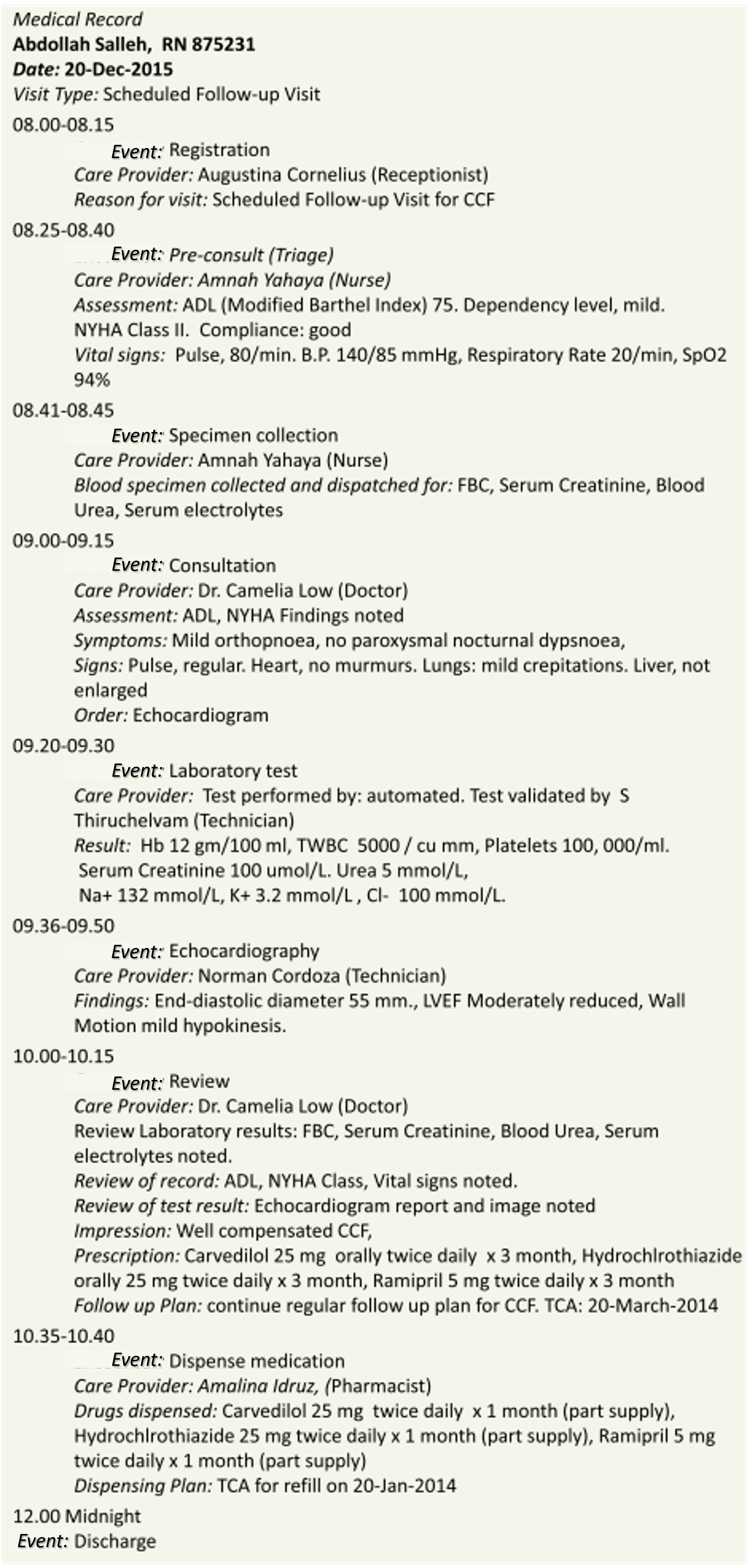
Example of Content and Arrangement of EMR for an Outpatient Visit
Content and Arrangement for an Episode
The basic unit of a medical record is data collected during a visit at a particular healthcare institution. To ensure coherence, data collected at multiple visits are also arranged in chronological order. Each visit is identified by the date and time, the care location, and the the type of service.
Traditionally, when paper records are used , the data are arranged by putting together data from different visits in two ways:
- All data for all health problems during a time period (the fully integrated Medical Record)
- All data pertaining to the care of the patient for a particular health problem (record kept separately by different departments or units)
The latter arrangement is convenient but unsound from the view of holistic care and continuity of care.
The CIS enables all data to be captured into and made available from a single database. From this fully integrated record, it is also possible, through a query of the database, to separate out data essential to a particular specialty or the care o a particular illness/health problem as views rather than an EMR. However, from a medico-legal standpoint, it is the responsibility of the health care institution to keep a record of data (Medical Record) for every visit at the institution and events that happen during that visit . Use of CIS and EMR and a common database puts a stop to record keeping by individual departments.
Supplementary Segments
Again similar to paper records, besides the temporal segments separate documentation may be provided as sections pertaining to a subject matter. This is indicated for multiple and repetitive findings where knowing trends and deviations are especially useful for example in case reviews. Each section is discreet and presented as lists or in tabular format with chronological sequence. These separate sections include:
- Monitoring parameters
- Lists of Procedures
- Medication given
- Laboratory results
- Diagnosis made (the Problem List)
Integrity of the Record
Each patient has a single integrated record relating to the services provided and the events that happen in the health care institution where he/she is being cared for. He/she is given a single medical record number which can be the same as patient’s unique identifier in the Patient Information Database when he/she registered as a client or another number (alias) mapped to it.
RECONCILIATION OF MEDICAL RECORDS
If for some reason more than one entity had been inadvertently created for the same person in the Patient Information Database and therefore the EMR, there must be a facility for the data belonging to the same person to be merged. Care must be taken to ascertain that the data belongs to that patient. This facility needs to be a front-end tool easily utilized by authorized person who can be record officers or IT personnel. There should also be a facility to unmerge the records if necessary.
Storage of Medical Records
The EMR of each patient, being extracted data derived from the operational database, is stored in a separate data repository primarily as a document with a defined content and structure. For most users it is mainly a read only document. Copies can be made available in a word processor document format, PDF or any other easily readable format. Being printable, hard copies of it can be shared.
PORTABILITY OF EMR OR PORTIONS OF IT
The EMR document is a good means of passing information from to a care provider to another provider that do not have access to the same HIS. It should be written and published in a standard portable document format (PDF, XML, Open document or XPS) readable by commonly used document reading applications (e.g. Adobe Reader or Microsoft XPS Viewer). Each EMR should be stored as a document file in a separate filing system and from where it can be downloaded and written to commonly available transportable storage media (USB drive, DVD-ROM, portable Hard Disk), mobile phone and printed on paper; or exported via a secure web area network. The same is true for visit or episode summaries.
Integrated Health Record (Lifetime Health Record)
The use of computerization and information management technology has enabled the pooling of data (complete or summarized) in a central shared database. Such records should include instances of visits to obtain services for:
- the management of the person’s diseases
- health promotion, disease prevention and early detection of disease (wellness services)
Increasingly, to facilitate the continuity of care across facilities, there is demand for data from all visits (whether from the same or different institutions) to be put together as the vertical medical record or the Lifetime Health Record.
Such a record are called variously the vertical health record of a person, the Lifetime Health Record or an Electronic Health Record (EHR). Access to records generated at visits at different institutions or a summary of it, enables the clinician to know the whole picture about each patient’s health and illness. This leads to better continuity of care. Such an arrangement require cooperation between institutions and another body to manage the shared database.

SECONDARY USE OF RECORDED PATIENT DATA
is discussed in another article.
Primary users of patient data are mainly care providers who would use the CIS to perform their work. Secondary users would be given privileges to use the EMR. The medical record data is used in two main forms i.e.
- Use of data from a single record
- Use of aggregated data
Secondary Use of a Single Record
A single record may be used in Qualitative reviews of the care of a patient for instances such as:
- Mortality or Morbidity Reviews
- Inquiries
- Quality audit
- Qualitative research
Because these are in-house activities, the CIS application may be used to sift through the record but an ongoing EMR would serve the purpose better. The most important use of Medical record is as a Medico-legal document. For this purpose the record need to be complete, presented in an orderly manner and easily understood.
Secondary Use of Aggregated Data
The medical record and the DBMS that supports it should be designed so as to allow the extraction and analysis of aggregated structured data for use by secondary users such as Managers, Quality Management, Record officers, Researchers) for purposes of:
- medico-legal inquiries (what went on, who were involved, when, where)
- review of entire care (audit, qualitative research)
- calculation of incidence/occurrence/prevalence for epidemiological and clinical research
- creation of registers,
- assessment of resource utilization,
- performance of audits,
- measurement of productivity / efficiency/ quality indicators
- risk assessment,
All of the above is done from the database rather than the EMR. For some purposes, it may be detrimental to extract data from the operations database. To serve this purpose, a duplicate copy of the CIS database is made and utilized as the analytical database.
To enable sharing of data, there should be technical data compatibility to enable flow across systems and where necessary across organizations and semantic data compatibility such that data is understood by all users.
This requirement is detailed further under the section on Data Extraction, Analysis and Interpretation.

Good day Doctor, Very informative and thank you for sharing the HIS insight. As Engineer by profession now I have more appreciation on how the health depart make use of Technology . We sometimes take it for granted what is happening in the background Health department space
LikeLike
Hey there, I am a huge fan of your blog! I really agree with this as I work as a medical assistant for a BPO provider.
LikeLike