
Date First Published: January 9, 2015
Date Last Revised: July 8, 2026
Introduction
The subject of planning in patient care services is complex both in scope and depth. I am discussing it in four separate articles i.e.,
- Planning Patient Care
- Structure and Function of Standard Operating Procedures / Clinical Care Plans (current page)
- Development of Standard Operating Procedures and Care Plans in Patient Care Services
- Documentation of Standard Operating Procedures (SOP) / Care Plans for Healthcare
- Implementing SOP/Care Plans in Clinical Patient Care
Through this article, I propose the concepts and function of the use of Standard Operating Procedure (SOP) in the planning of the delivery of patient care. I belief that healthcare services should adopt SOPs as applied both in manufacturing and service industries worldwide. I also belief that the term Care Plans is synonymous with SOPs. Both are plans on carrying out the delivery of services. I will clarify the terms used when applied to patient care service and define the content and structure.
As a healthcare professional, I have also tried to apply the concepts through various projects with some success. There were many false starts I will try to express my understanding the subject. Readers, trying to get through this article may find it quite daunting. There are repetitions, and for some content, details are spread over a few sections. I have tried to present it as simply as is possible. I have gone to great lengths to explain the work of a clinician because readers are likely to include non-clinicians ranging from managers, administrative staff and people involved in information management. All need to understand each other’s work. However, a SOP is designed to improve consistency and therefore details are necessary. I hope you will bear with me and persevere in trying to go through reading it.
The design and implementation of SOP/Care plans is further elaborated in a separate article.
PRINCIPLES AND CONCEPTS
When used in manufacturing industries, the Standard Operating Procedure (SOP) describes the plan for the work of producing a product. The entire method of production is also termed as ‘operations’ which consists of a set of units of work called ‘procedures’. The term ‘standard’ refers to the uniform way that workers are expected to carry out the procedures. The SOP describes rather rigid methods, and the product has specific characteristics or specifications.
The product of services can also have fairly uniform characteristics and be called service products. Therefore, SOPs can be equally applicable to describe the operations of producing a service. Instead of production, we use the term ‘service delivery’. In both the aim is to ensure uniformity and consistency by conformance to standards. The difference is that service delivery methods are often adjusted (customized) to needs of the client and therefore more flexible. need to be documented.
Terms used in SOP
| Term | Meaning |
|---|---|
| operations | the entire effort of producing a product or delivering a service |
| product | the useful outcome (object or benefit) of an effort (work) |
| processes | the most elementary unit of work |
| procedure | tasks, a series or set of processes |
| standard | the common way to conduct an operation |
| SOP | description of the proposed/prescribed way of the work of producing a product |
Currently, there is an increasing awareness worldwide of the need to regulate healthcare services, streamline health care funding and ensure uniform quality of care. This has resulted in wider acceptance of the use of standardized documented plans. In many instances, the initiatives are driven by the need to be accountable. For example, organizations who provide funds for health care now determine or at least influence, what (input and processes) goes into the management of different types of cases and allocate funds accordingly. Accreditation bodies also expect healthcare facilities to have documented policies and procedures. Healthcare facilities are also expected to show whether the outcome of their services achieve acceptable standards.
| TERM | MEANING |
|---|---|
| Uniformity | the consistently similar manner by which services are provided for defined patient groups (case types) affected by the same disease, illness, or health problem. |
| Standardization | the use of agreed specifications for resources, processes, and outcome including the terms used to describe them. |
| Customization | making slight alterations through additions or omissions depending on conditions or situations |
Standard Operating Procedures in Manufacturing vs Service Industries
In manufacturing industries, the Standard Operating Procedure (SOP) describes the plan for the work of producing a specific product (item, object or goods) based on clearly expressed needs of the intended clients. The product, as well as are the input and processes used, has well defined specifications. The production system uses rigid methods that can be replicated easily at different sites. The activities are usually performed in a logical sequence. For some of the activities, the processes must be strictly continuous e.g. in an assembly line. Other activities such as processing of the raw material, fabrication of parts, assembly, testing and distribution can be done concurrently at separate facilities. Many of these methods cannot be applied to service industries.
Service Products
Like manufactured products, the products of services can also be described by equally uniform characteristics and outcomes. The outcome can be called ‘service products’ for the delivery of which SOPs can also be designed. Generally, in service industries including healthcare, the specifications of the service need not be defined very strictly. Often, there is a need for the delivery to be customized and personalized to fit the special needs of the recipient. The healthcare provider may be allowed to exercise discretion and vary both the input and processes and therefore the outcome.
Requisites for the Use of SOP in Healthcare
A SOP must match the capability of the organization. Hence when, building the SOP, the following factors must be taken into consideration:
- the aim of the organization in providing the service,
- the environment within the organization,
- the resources available,
- how the delivery of the service is organized
If the organization intends to improve the capacity or quality of its services, it must upgrade the above requirements. This means that each facility or organization must create its own sets of SOPs.
There is a need to demonstrate that these plans are feasible and effective through trial or pilot studies. Before being adopted, it should be verified by the managers responsible for governance of the services and formally endorsed by the executive body of the organization. After adoption the feasibility and outcome must be constantly appraised and improved upon.
Healthcare as a Service
‘Healthcare’ is the delivery of services aimed at:
- keeping persons healthy
- preventing diseases
- caring of people when they become sick
The term used for the provision of health services is ‘care’. Hence, the industry is called ‘healthcare’ and the workers in the industry are known as ‘care providers’, healthcare workers’ or ‘healthcare professionals’.
Care of the Sick
The provision of services to people who are sick is termed as ‘patient care’ or ‘clinical medicine’. Often, it is also called ‘curative medicine’ (incorrectly, since cure is not the aim in all cases).
Services for the Healthy
The services of keeping persons healthy follows a different approach (the wellness paradigm). It is concerned with:
- promotion of health
- prevention of disease
- early detection of disease
These services are delivered to a different set of clients and use different resources and methods. The design of the SOPs / Care plans will be different.
The Wellness Services and the use of SOPs/Care plans in them will be described (hopefully) in separate articles.
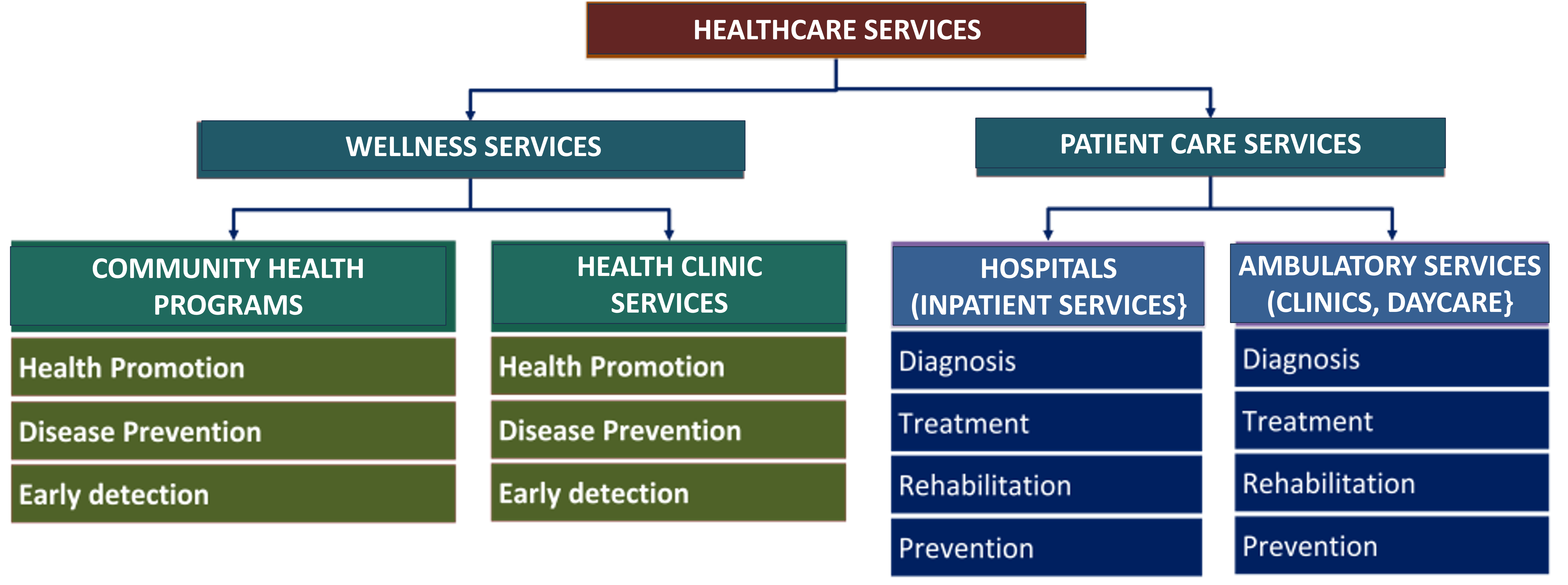
SERVICES OFFERED BY A PATIENT CARE FACILITY
A healthcare facility offering patient care services encompasses two main group of activities, functions and services i.e.:
- Managing the patient care facility as a business entity, a provider of hospitality services and a physical facility
- The core business of providing patient care services
Managing the Facility
Patient care as a service require complex resources and methods. The viability of health service delivery facility requires attention to optimization of costs. Those depending on funds or grants by the government or charity must work within the budget allocated. Facilities whose expenditure depends on money accumulated from payments, whether made directly by patients or through insurance schemes, must take into account affordability and competitiveness. The SOP supports the framework for the calculation of costs because it details out the processes performed, the resources and the environment required to perform them. I will devote an entire article on the subject of costing, charges and funding.
Provision of Clinical Care
The Patient Care Service itself consists of:
- clinical patient care i.e. the services provided by care providers involved directly in looking after patients (clinicians),
- the administrative aspects facilitating clinical care (administrators, clerks, receptionists),
- services that support clinical activities (laboratory, imaging, endoscopy. etc.)

SOPs for Administrative, Supportive and Facilitatory Aspects of Patient care
Some aspects of patient care services are not very different from other services in as much as they have fairly uniform output characteristics. These services have fairly clear policies and procedures which are quite similar to that used in industries. Applying SOP in them is not difficult. It has been tried for some time with success. Also, the policies and procedures can be followed fairly rigidly. Such areas include:
- Management functions and services
- Client (Patient) Administration services (i.e. registration, scheduling appointments, resource allocation)
- Clinical support services (e.g. laboratory, imaging, endoscopy, sterilization),
- Ordering and supply of resources (drugs. blood products, instruments etc.)
- Work assignment (Rostering, worklists, schedules)
The service provision for administrative, supportive and facilitatory aspects of patient care is not very different from those in other services. SOPs have been used successfully in these areas.
Applicability of SOPs in Patient Care Services
The design of SOPs for clinical patient care is unique. The effort required for achieving uniformity and standardization is more demanding. Currently, clinical care providers including doctors, nurses, allied health personnel and other professionals follow universally agreed approach to delivering care. The challenge is the need to provide a wide variety of service products to match various types of diseases and their variants. Yet, it is the patient and not the disease that care providers are concerned with. Hence, the service must take into consideration the individual needs the patient. A clear understanding of principles, concepts and methods used in patient care is required if SOPs are to be developed.
Challenges in Using SOP for Clinical Patient Care
The applicability of SOP in the direct care of patients by clinicians is less clearly worked out mainly because of the wide variety of illnesses, diseases and health problems. However, currently there is a realization among managers and clinical care providers including doctors, nurses, allied health personnel and other professionals on the need for standardization. Foremost among these is the effort by professional bodies generate consensus via the development of Practice guidelines.
Modification of SOP/Care Plans for Different Facilities
The facilities that offer patient care services include:
- Hospitals (with inpatient and outpatient services)
- Stand-alone clinics or polyclinics (outpatient services)
- Daycare centers
Obviously, the way service is delivered varies with the type of facility and design of SOP/Care plans must accommodate accordingly.
Diagnosis as the Main Criterion for Differentiating Service Products
Patients. Cases. Clients. Service products must be provided for many types of illnesses, diseases and health problems and therefore SOPs have to be developed for service products to correspondingly match these wide variety of needs. The type of disease and the need of the patient is defined predominantly by the diagnosis. Hence, service products and their SOPs must be developed based on diagnosis.
The objective should be to retain and apply the common principles, concepts and methods of patient care for each one of them while giving due consideration to the special needs of each type of case. Yet, it is the patient and not the disease that that the service is being provided for. So, there must be a method for modification and customization of the SOP to cater for the special needs of each patient.
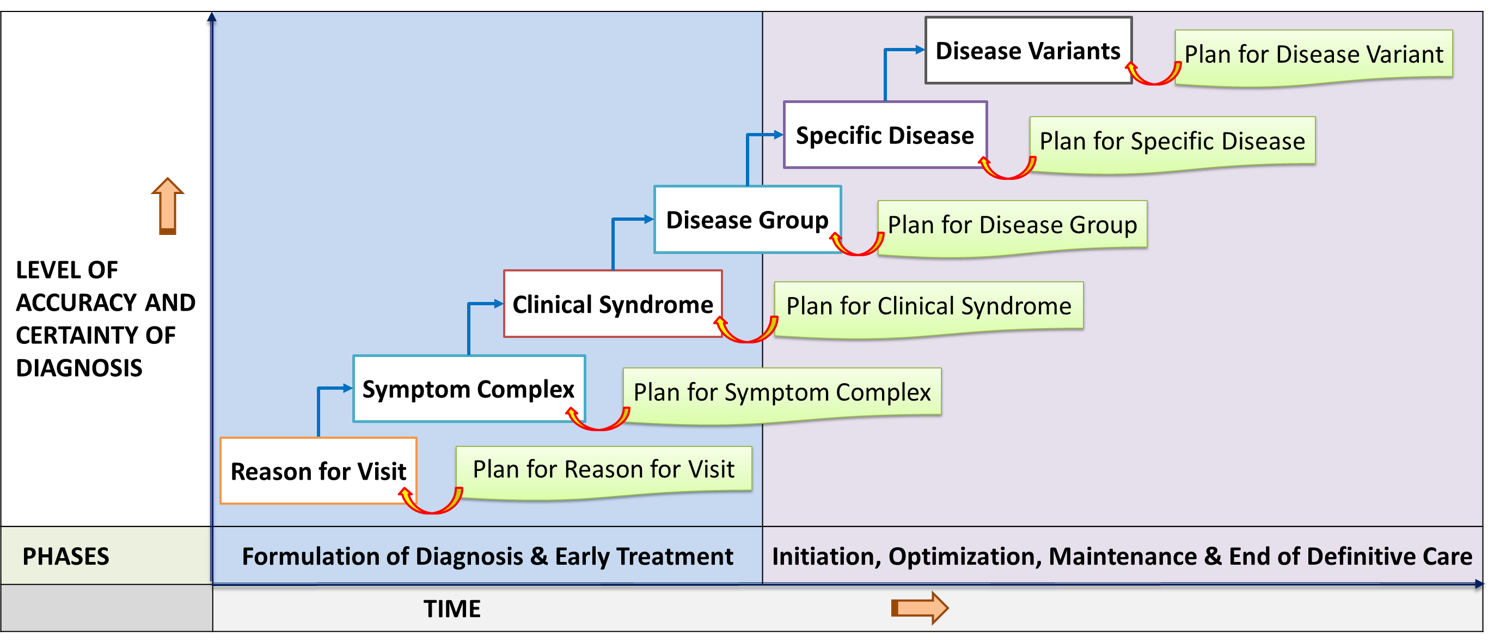
In summary, Clinical Patient Care services are provided according to the patient’s illnesses, disease or health problem as defined by the diagnosis. Since there are many types of diseases, there are corresponding wide varieties of service products. It must be remembered that the diagnosis becomes clearer as the care process progresses. Hence, SOP/Care plans must be designed for the early phase (symptom complexes, clinical syndromes) as well as the later phase (specific disease and its variants).
Preferably, SOPs must be made available for all of them. This would be a tremendous challenge, but I propose that the use of the Standard Operating Procedure (SOP), is not only applicable but also necessary.
- phases according to the theoretical application of the clinical care processes
- breakdown of services into practical blocks of activities (sessions, time slots).
SOP vs CARE PLANS
Many attempts has been made to develop proper methods of planning in patient care. Currently within the healthcare community, the design of the service for a typical patient with an episode of a specific illness is often called the ‘Plan for the Management of a Patient’, ‘Case management protocols’, Care bundles, ‘Care Plan’ or ‘Care Pathways’. There are many conceptions and formats of what is called ‘Care Plans’. It is common to depict the Care Plan as a table or matrix. This is not the best way to express it because tables limit the amount of content and do not show sequence and layout clearly. It is better for the content of patient care plans to be in structured narrative format similar to the SOP used in other industries. The term Good Clinical Practice (GCP) is also used but unfortunately it is only applied in research settings. Despite its name, it is not concerned with proper clinical care but on how to conduct a clinical trial.
Both the Care Plan and SOP refer to the predicted or planned policies and procedures in managing a problem. If the the same methods, structure, and content as used in developing ‘Standard Operating Procedure (SOP) in other industries is adopted, with some modifications, then the Care Plan and SOP can be seen as equivalents.
If it is more acceptable, the term Care Plan can used in lieu of the term SOP. In practice either term can be used interchangeably. Henceforth in this discussion, the SOP and Care Plans are deemed to be synonymous. Both terms will be used together abbreviated as SOP/Care Plans.
The way to develop and document SOP/Care Plans is discussed in another article.
FUNCTION OF THE SOP/CARE PLAN
SOP/Care Plans provide the guide to care providers on the work to be performed to produce a product or to offer a service (a service product) and the policies that govern them. The basic contents are packages of tasks bundled together, arranged, and sequenced according to the workflow. The overall plan provides direction to the clinician on tasks to be performed for a patient, from the beginning to the end of the care episode. It is then further broken up into sections for various sessions, phases, visits, and events within the episode.
Each SOP/Care Plan describes the plan for the realization of a specific service product i.e., the care of patients with a particular disease or health problem. There should be an SOP/Care Plan for every service product. Each one has the following functions:
- explain the theoretical basis for the way of the service is delivered
- ensure that service providers adhere to policies and procedures
- help care providers make the right decisions
- act as a source of knowledge to help the care provider give safe, effective, and appropriate care.
Hence, the SOP/Care Plans can act as reference document for use as:
- the guide to carrying out work
- resource material for training
- the standard for comparing actual performance with what is expected
Technical Difficulties in Implementation
The technical difficulties in applying SOP methods to patient care stem from two main factors:
- there are wide varieties of service products each with varying policies and procedures
- the workflow in patient care is not exactly sequential, it is often iterative.
The clinical care process is generally sequential but certain criteria must be met for the workflow to move on. Often repetitions of processes or procedures are necessary. The cyclical or iterative nature of clinical care need to be understood and incorporated into the SOP.
Also in many instances, the care or even part of the care cannot be completed at one sitting due to time constraints or the need to wait for outcome or results. The delivery of care needs to be broken up into:
Because of the above factors use of SOPs/Care Plans in clinical patientcare must follow a two-step process i.e.
- a suggested framework
- adaptation of the framework to the current case
SOP/Care Plan as Reference vs Actual Plan
For a start, the SOP/Care Plans can be taken to be a detailed plan applicable to the delivery of services to typical patients affected by a typical disease condition (the service product) in a particular facility or organization. As in any other service, the design and planning of clinical care involve translating the needs of particular recipients (patients) into uniform specifications and standards of both the service delivery itself and more importantly the final outcome of the service. In practice this documented plan is a Reference Plan.
Almost invariably, customization of the SOP/Care Plans would be necessary when the actual care is to be provided to an individual patient. variance
Moving Away from the Traditional Way of Planning in Clinical Patient Care
The traditional way planning as practiced in patient care differs significantly from the approach in industries. In clinical patient care, based on the SOAP approach, the planning process occurs after the diagnosis has been made.
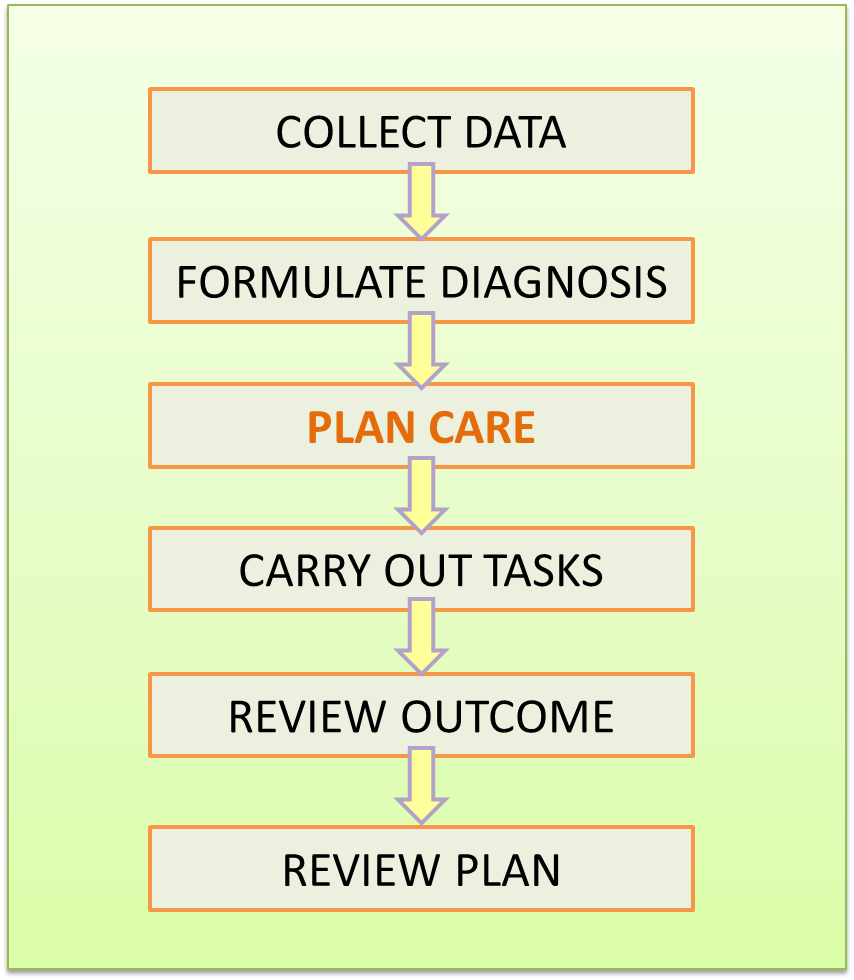
In the industrial setting, the scope of planning encompasses all activities from the very beginning of production. Industries use the SOP as a plan that describes the entire method (operations) of producing a product or delivering a service. Hence, instructions are provided for actions to be taken from the very beginning. This is unlike the traditional thinking in clinical medicine where planning is thought to happen after the diagnosis has been made.
The Better Approach to Planning
Planning should be a preparatory series of thought processes that are then documented. The steps as applied to all types of services and service products should be as follows:
- Identifying the case type and the service product
- Determining the objectives of care
- Deciding on and choosing the approach and method
- Deciding on the sequence and layout of actions and scheduling them
- Ensuring that resources are available to carry out the plan
- Assigning responsibilities
- Anticipating issues that may arise
- Documenting and communicating the plan
When building the SOP for an organization, the following factors must be taken into consideration:
- goals of the organization in providing the service,
- the environment existing within it,
- the resources available and its readiness
- how service delivery is organized
Managers of healthcare facilities are concerned with the viability of the service and therefore are focused on efficiency and cost-effectiveness. Clinicians on the other hand are interested in the effectiveness, appropriateness and comprehensiveness of the care given. The SOP must address all these concerns.
Defining the Characteristics of the Service Product in Patient Care
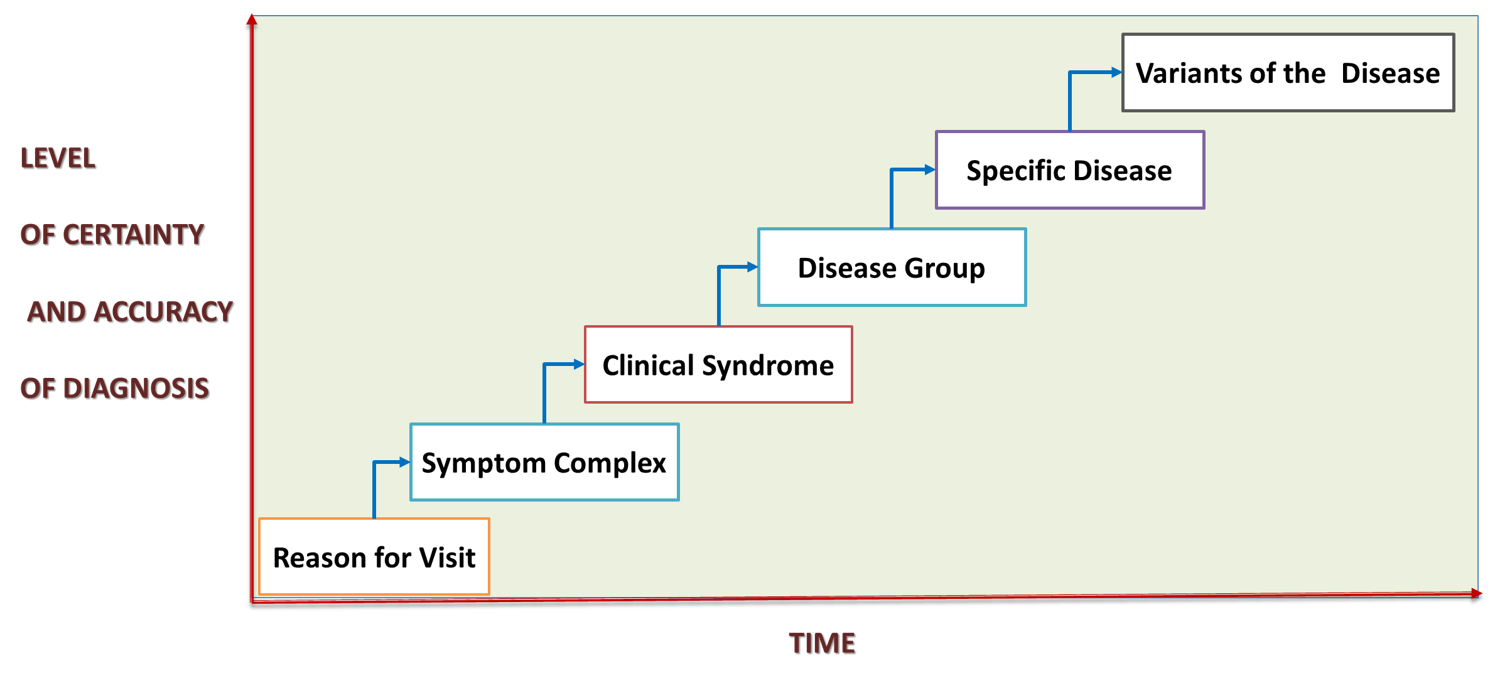
To apply the concept used in industry to patient care, it must be assumed that a service is offered to the patient as soon as the person seeking care arrives at the facility. If possible, the service to be given is inferred at the moment of registration or immediately after it. For new cases knowing what service to provide is a challenge. Yet even at the start, the diagnosis can be determined by fashioning it around the reason for visit even if it takes the form of symptoms or complaints. The set of symptoms (symptom complex) supplemented by the discovery of certain signs that are obvious on observation or through simple assessment (at triage) can be taken as a preliminary diagnosis used to infer the needs of the patient and the service that they should be provided. If the preliminary diagnosis is expressed in a standardized way as properly named symptom complexes and clinical syndromes, then the service product and hence the SOP for it can be determined from the very beginning. In this way appropriate general care plus symptom relief, and supportive therapy can be given from the start. The difference (as will be discussed later) is that the characteristics of the service product changes as the diagnosis becomes clearer.
Services in patient care are numerous and diverse. The challenge here is to define the service products to be offered and then design the SOP/Care Plan for each of them.
Diagnosis as the Main Criteria for Differentiating Service Products
The Range of Service Products in Clinical Patient Care
The subject of the levels of accuracy and certainty is discussed in the article entitled Formulation of diagnosis.
Design of Standard Operating Procedures in Patient Care
When consolidating the design two aspects have to be looked at:
- what procedures are to be done and in what way
- how the above is to be documented
What procedures are to done and in what way must be thought out first by the persons responsible for the design. For it to be understood and followed it must be documented and made available as a written SOP/Care Plan. The content and structure of the document must then reflect the way the service is to be delivered. However, once the document is made available it becomes the the authorized guide for all care providers in the facility to follow.
Documenting what is to be done —-> Carry out what is documented
The outline of the steps to be followed by an institution or facility when developing SOP/Care Plans is outlined below:
- Identify the clients and any variations in their needs
- Identify the Service products to be offered.
- Define the expected outcome,
- Propose the service delivery system
- Propose the policies and procedures to be followed
- Outline the layout and sequence of tasks (Workflow) including alternatives where necessary
- Allocate responsibilities (organization of the care team, work schedule, task lists)
- Define the control limits of both processes and outcome (policies)
- Incorporate methods to ensure compliance with them (built-in Quality control),
BENEFITS OF THE USE OF STANDARD OPERATING PROCEDURES / CARE PLANS
The use of a SOP/Care Plan for the care of a patient with an identified disease condition or health problem (a service product) confers benefits for health care providers and health services managers alike. In the end, patients would greatly benefit from care that is made consistent and controlled.
Achieving Uniformity and Standardization through SOP/Care Plans
SOP/Care Plans can be used to establish greater uniformity and standardization in the delivery of care. This is of benefit to the healthcare profession as well of the facilities that provide patient care services.
Benefits to the Healthcare Profession
SOP/Care Plans will benefit the healthcare profession as a whole by promoting:
- evidence-based practice
- common objectives and methods
Healthcare providers will be encouraged to abide by policies and procedures that is based on sound theory and experience (research, consensus and best practices). The sharing of common objectives and methods will enhance mutual understanding and reduce conflicts.
Benefits for the Care Provider
For the care provider, formalized planning of care provides many advantages including:
- Facilitate care that follows a more structured plan
- Include comprehensive content
- Encourage proper choice of investigations and treatment (remove redundancy / duplication and wastage)
- Promote better resource utilization
- Provide information and decision support (prompts and reminders)
- Give a clear picture of future actions
- Communicate intentions to the care team (shared objectives and understanding, create task lists)
The SOP/Care Plan acts as the guide for the care provider in the care of his/her patients by providing the essential knowledge on the selection of approaches, paths, methods, and standards. It is therefore a good tool for staff orientation and training or as a reference source when in doubt. The degree of detail within it means that it has to be studied conscientiously to be understood. When implementing a SOP/Care Plan, it is assumed that the care provider is conversant with its purpose, content, and structure. The rationale, objectives and methods need not be presented in detail but referred to (through links or appendices) or summarized. In addition, when performing specific tasks, instructions and specifications that are precise and didactic are required. These are provided as reference documents such as Work instructions and Reference tables.
Benefits from an Operations Management Perspective
From an Operations management perspective, a documented SOP/Care Plan is useful for the following purposes:
- Provide information, guidance, and decision support
- Clarify objectives and targets
- Facilitate conformance to prescribed approaches and methods
- Be the standard/specifications for quality measurement and control
- Act as a guide for staff orientation and training
- Provide predictability in resource planning (staffing, facilities, equipment, technology and information)
- Form the basis for the development of information systems
- Provide a rational basis for costing and charging
Benefits For the Unit or Department Manager
For a service or department manager, the use of SOP/Care Plans can lead to the following:
- Promote uniformity and standardization
- Render a degree of predictability in the supply of various resources
- Act as a basis for quality measurement and control
- Encourage equitable care and remove bias
- Improve staff knowledge, skills, attitude and behavior
Benefits From the Business Perspective
From the perspective of providing a service, the SOP/Care Plan defines the package or bundle of tasks and input that make up a service product. Charges or the funds required can be calculated by costing the type and number of tasks to be done, the degree of difficulty, the time taken and the resources (workers, facilities, equipment and raw material) required to deliver the service. Indeed, currently many funders such as insurance companies and government agencies rely on care plans to justify claims or to advance funds to facilities. Reduction in costs by the use of care plans has been shown in one study.
Benefits From The Strategic Management Perspective
From the perspective of strategic management, SOP/Care Plans provide the foundation based on which changes and improvements can be made, and benefits evaluated. A clear example would be the re-engineering of processes when computerized information technology is introduced. Without documented SOP/Care Plans, the current and earlier practices cannot be compared and it would not be possible to distinguish any improvement. Software developers develop applications that facilitate care providers to do their work by depending on workflows to write programmes.
Standardization of procedures allow the accumulation of more reliable data that can be used to determine use of resources and the achievement of targets (success and failures). The information can be used to predict trends and enable planning.
OVERCOMING DOUBTS ABOUT USE OF SOP/CARE PLANS
Despite these benefits, there are apprehensions, among clinicians and managers alike. Many worry that that use of standardized plans will lead to:
- people following them blindly (“cook-book” medicine)
- loss of clinical freedom
- may be misused in medical negligence litigation.
The first concern is valid and should be addressed by building in variations, exceptions, alternatives and contingency plans into their design.
For the second concern, it must be stressed that the SOP/Care Plan, when first designed, is a reference document to be used as a guide. It has to be converted to actual plans with active input from the healthcare provider in charge of the case him/herself before being applied to actual care.
Medical negligence is defined as “an act or omission (failure to act) by a medical professional that deviates from the accepted medical standard of care”. The worry here is that the SOP/Care Plan can become the de facto medical practice standard. The argument usually made is that documented the SOP/Care Plans make the standard too certain whereas without it the criteria for negligence lack certainty and thus provide leeway for defense. Clarity should be welcomed. Currently, the term evidence-based medicine is the by-word for the accepted way. Yet, the term ‘evidence’ itself need to be clearly defined. It should not be construed as only what transpires from research or what is printed in journals. SOP/Care Plans may be a better basis for defining the acceptable standard because it considers the practical aspects of practice in a specific work environment taking into consideration the limitations that exist. Indeed, information derived from actual practice (best practices) have value that research do not provide.
Most medical practitioners (except for those in lone practice) work in a facility where they are dependent on other care providers. In fact, the facility is as liable to claims of negligence as the practitioner. There is a need for the facility to advocate common policies and procedures and provide it as SOP/Care Plans. Making them available is part of good governance. If they are designed based on scientific knowledge, research findings, best practices, consensus, and experience, they act as a deterrent for practitioners from unacceptable practice and a shield against frivolous litigation. However, not following the SOP/Care Plan to the letter should not be construed as deviating from the norm. The care provider is allowed to modify elements of the SOP/Care Plan based on his/her own judgment when faced with certain situations. It is advisable to record and explain the reason for the variance from prescribed policies and procedures.
Ensuring Validity of SOP/Care Plan
There is a need to demonstrate that these plans are feasible and effective through trial or pilot studies. Before being adopted, it should be verified by the persons or committee responsible for Clinical Governance and formally endorsed by the executive body of the organization. It must be audited to confirm its applicability and continually updated.
For the SOP/Care Plan to remain valid it must be continually updated. The people in charge of producing them need to be constantly aware of recent developments.
Also the healthcare facility need to ensure their dissemination and adherence to them. It must also review their effectiveness in achieving intended objectives. The best way is to audit the use of SOP/Care Plan. Findings from the audit is then used to improve conformance as well as to rectify the structure and content of SOP/Care Plan itself.
Therefore, when using a SOP/Care plan as a guide, the planning process is done in two major steps i.e.:
- Choosing the appropriate Reference (Model) Plan from the library of previously prepared care plans
- Converting the chosen reference plan into the actual plan by customizing it to cater for the special needs of the patient
Use of the SOP/Care Plan as the Reference Plan
At the beginning, the efforts must be made within the healthcare facility to design standardized operating procedures or care plans that are generic in nature i.e. applicable to typical patients with a typical disease condition (rather than an individual patient). There should be an SOP/Care Plan for every service product. To that end, the structure should follow closely the clinical processes. All such plans should be made available for reference (by whatever means) as a properly indexed comprehensive library of documents. The Reference plan for a particular case is selected from this library.
All aspects of care must be addressed at the time of the development and design of Reference Plans. As far as possible all objectives (outcome), policies and processes are thought out, eventualities anticipated, and variations considered. As the care of a patient is a multidisciplinary effort, each professional group should be involved. For example, a section for nursing care should be included in the Reference plan. It should address the aspects of nursing required for the disease, illness, or health problem for which the plan is written. There should not be a separate Nursing Care Plan standing on its own. The same is true for plans for rehabilitation or the care for psycho-social issues. This is in contradistinction with current practice.
Conversion of Generic SOP/Care Plans for Use on an Individual Patient
Variety Of Service Products of Clinical Patient Care
The need of the patient as a client is expressed less clearly than that in other services. While the typical disease as described in a textbook usually encompass all presentations of it, different categories and variations of the disease may be considered as different service products.
Interpreting the nature of the health problem inappropriately and therefore choosing an inappropriate plan would lead to dire consequences. Because of this differentiation, when documenting the SOP/Care Plan consideration must be to the situations:
- when the difference is significant enough for a separate SOP/Care Plan to be designed
- when different styles, content, and structure are required
Building SOP for Different Types of Service Products
Firstly a SOP/Care Plans is designed such that the service given is adjusted to cater for the practices peculiar to patient care. Hence, well accepted and proven approaches, methods and tools already in use in health care must continue to be applied.
Next , SOP/Care Plans contains a defined set of services making up the care for a patient affected by a typical disease, illness or health problem. It is designed to cater for needs determined largely on the identified diagnosis.
Additionally, plans must be prepared for the variants of the disease as:
- sub-sets, extensions or appendices to this main SOP/Care Plan.
- separate distinct plans if the variant need to be cared for differently.
If the SOP/Care Plan conforms to the universal practice of patient care, they can be applied at any facility except that they will have to be modified to suit its capability.
Flexibility in Design
Diagnosis as the Primary Basis for Design of SOP/Care Plans
A SOP/Care Plan is designed for a service product which in turn is defined primarily by the diagnosis. Clinicians use the term Working diagnosis to denote the best diagnosis that can be deduced at any point. The best diagnosis here refers to the degree of certainty of the diagnosis based on the information available. This is the diagnosis that form the basis for the design of the SOP/Care Plan at any current phase of care.
At the initial phase of care, based on clinical experience and study, the diagnosis for some health problems can be made with high degree of certainty by relying on the presence of certain symptoms, signs and results of simple point of care investigations. In other words, the diagnosis is obvious and is often termed as the “spot diagnosis”. In this situation, a comprehensive plan for the case can be chosen and adopted.
However, for most other cases, the diagnosis at the initial phase is less clear. Yet for some, the information available allows the clinician to assign the patient to the diagnosis of known symptom complexes, syndromes, or Diagnostic Related Groups (DRGs). A symptom complex or syndrome are disease conditions that have typical set or pattern of manifestations (group of symptoms, signs and test results) attributable to diseases affecting a particular body region, a physiologic system or of a particular aetiology. Such diagnoses even though not totally clear can be exploited for the following benefits
- narrow down the differential diagnosis to diseases pertaining to an anatomic region, a physiological system or a causative pathology.
- give pointers to what to do next (e.g. more detailed interview, clinical examination and type of investigations to be performed).
- allow for certain treatment to be initiated e.g. symptom relief, preventive actions, general or specific supportive measures.
It is the common manifestation of many possible diseases (e.g. Obstructive jaundice, Bleeding disorder and Upper Gastrointestinal Bleeding).
There is a substantial proportion of cases where the diagnosis is unclear or uncertain. The reason for visit may be vague symptoms or symptoms and signs attributable to a wide variety of illness, or generalized feeling of ill health that does not point to disease of an organ or physiologic symptom.
Subsequently, as more information is available, a different diagnosis may be made.
Hence, it is not good enough to continue using the SOP/Care Plan based on As the amount and quality of data is available to the clinician increases, the working diagnosis becomes more accurate changing from a broad or general diagnosis, to a provisional or presumptive diagnosis and then to a definite diagnosis. This effort at ascertaining the most accurate and certain diagnosis occurs mainly in the early phase of care. At this phase the diagnosis can be initially uncertain expressed as symptom complexes, clinical syndromes and disease groups or certain (definite) expressed as specific disease.
Even if the diagnosis is considered as definite, developments in later phases may point to more accurate diagnosis such as variants and sub-types of the disease. Certain contingencies may happen that will necessitate changes in the care plan.
Illness, Disease and Health Problem
Persons who are sick are affected by ailments that by convention are loosely categorized into illnesses, health problems or specific diseases.
| TERM | MEANING |
|---|---|
| Illness | The feeling that something is not normal about a person’s health. It may be part of a disease, which may still be undetected. Symptom complexes and clinical syndromes can be considered as illnesses. |
| Disease | A specific condition of ill health distinguishable by a known set of criteria that can be a mix of: — clinical manifestations, — underlying pathological process detected through tests or — observed behavior. Disease usually show up as illness. However, they can also exist without any obvious manifestation (latent, dormant, asymptomatic) and detected through tests. |
| Health problem | A condition where a person’s well-being has deviated from normal in function or appearance. It can be: — part of an illness, — an infirmity, disability. deformity or malfunction, — physiological changes (e.g. pregnancy, malnutrition). |
Reference SOP/Care Plans should be constructed for all entities within these categories. They are compiled, indexed and kept as a set of reference documents which, when properly indexed, are referred to in industry as the Work Procedure Manual. Each document consists of various components that address various aspects of care (written as sections and paragraphs). The components would be like those in SOP already in use in other industries as will be outlined below.
Appropriate Plans for Different Levels of Accuracy of the Working Diagnosis
From the perspective of developing SOP/Care Plans for service products, ailments must be categorized more objectively. This objectivity depends on the levels of accuracy of the working diagnosis.
It is often thought that SOP/Care Plans can only be designed for when a specific disease has been diagnosed. This is not true because care must be instituted even when the definite diagnosis has not been identified with certainty. The plan for the service to be offered to the patient must be made available as soon as the patient seeks care at the facility.
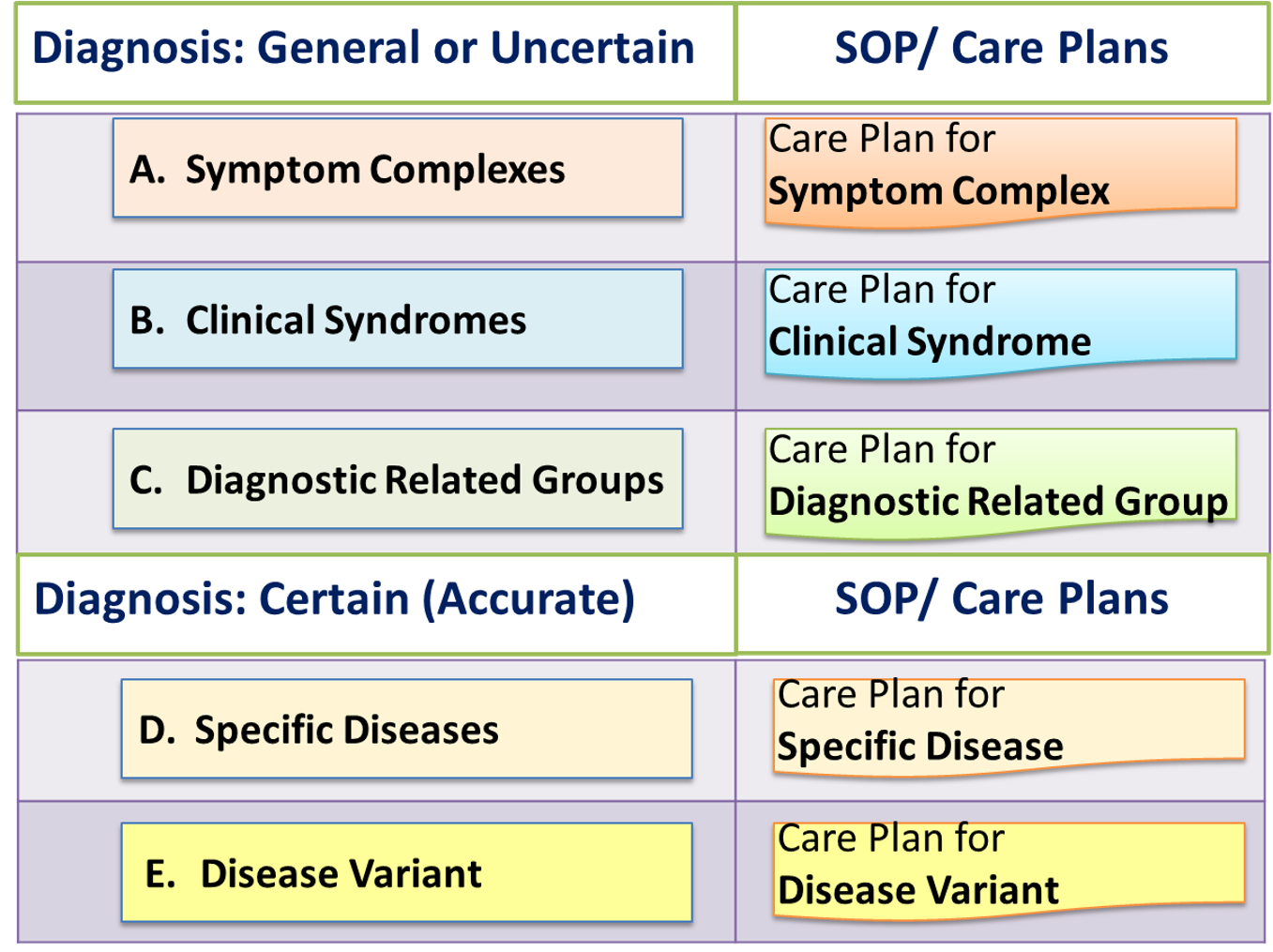
Levels of accuracy of the working diagnosis increases as the patient care process advances through its phases. The characteristics of the service product changes at the different levels of accuracy of the working diagnosis. Hence, SOP/Care Plans must be created for the care of patients diagnosed at these levels of certainty i.e.:
- When the diagnosis is general or uncertain
- When a specific disease has been identified
The primary care provider (usually the doctor in charge) is the person responsible for arriving at the diagnosis. Therefore, he/she is also the person to select and initiate the care plan and to change it as the care progresses.
The service product can be named after entities corresponding to these wide range of diagnosis using accepted terminology e.g., derived from ICD-10 Classification of diseases or SNOMED. As the diagnosis changes different service products will be offered to the patient. The various types of service products will be discussed further below.
PLANNING WHEN THE DIAGNOSIS IS GENERAL OR UNCERTAIN
The nature of the illness affecting the patient is not immediately apparent at the beginning of patient care. The diagnosis evolves with accumulation of data gathered through interview, examination and simple tests. This happens at the early part or phase of care where the focus of care is on gathering data to determine the diagnosis and to provide the pertinent immediate treatment
At the beginning or early phase of care, the illness as expressed by the patient can be identified as a group of symptoms termed as a symptom complex. The pattern of symptoms provides a pointer as to the scope and direction of further information gathering for the purpose of clarifying the diagnosis and gauging the general status of the patient.
At this point, the main concern of the service is relief of symptoms and provision of support. Subsequently, when signs are elicited and results of simple tests are obtained, the patient can be placed into a group termed as a clinical syndrome, or a diagnostic related group, Clinical syndromes are characteristic of certain categories of diseases. From the the mix of information, the care provider can infer the possible underlying disease (the differential diagnosis). At this point, care addresses various problems common to the group and care is given corresponding to it.
Therefore, it is necessary to build SOP/Care Plans for these broad diagnosis expressed as:
symptom complex,- a clinical syndrome or
a diagnostic related group.
These SOP/Care Plans contain actions required to address the general needs of the patient no matter what the definite diagnosis would be. They would be applicable at the early stage or phase of care. The care processes at this phase of care is shown in the table below:
| Working Diagnosis | Objectives | Plan and Content |
|---|---|---|
| A. Symptom complex B. Clinical Syndrome C. Diagnostic Related Group D. Clinical Syndrome | a. Symptom relief b. Resuscitation c. Stabilization d. Obtaining sufficient data | Care plan to a. Determine Diagnosis — Gather Clinical data — Investigate b. Early Treatment — Relief symptom — Restore function — Stabilize |
Definitive care will be given only when the definitive diagnosis is arrived at. How these would be used at the early phase of care will be discussed later.
SOP/Care Plans For Symptom Complexes, Syndromes And Diagnostic Related Groups
When the diagnosis is expressed as Symptom complexes, Clinical syndromes or Diagnostic Related Groups, the SOP/Care plan contains activities aimed at:
- clarifying the diagnosis further through diagnostic investigations
- providing treatment for symptom relief
- providing supportive therapy (resuscitation, stabilization)
- establishing monitoring and observation routines
introduction of preventive measures and rehabilitation
These activities occur at the early period (phase) in the of the care episode. They will be discussed in detail later.
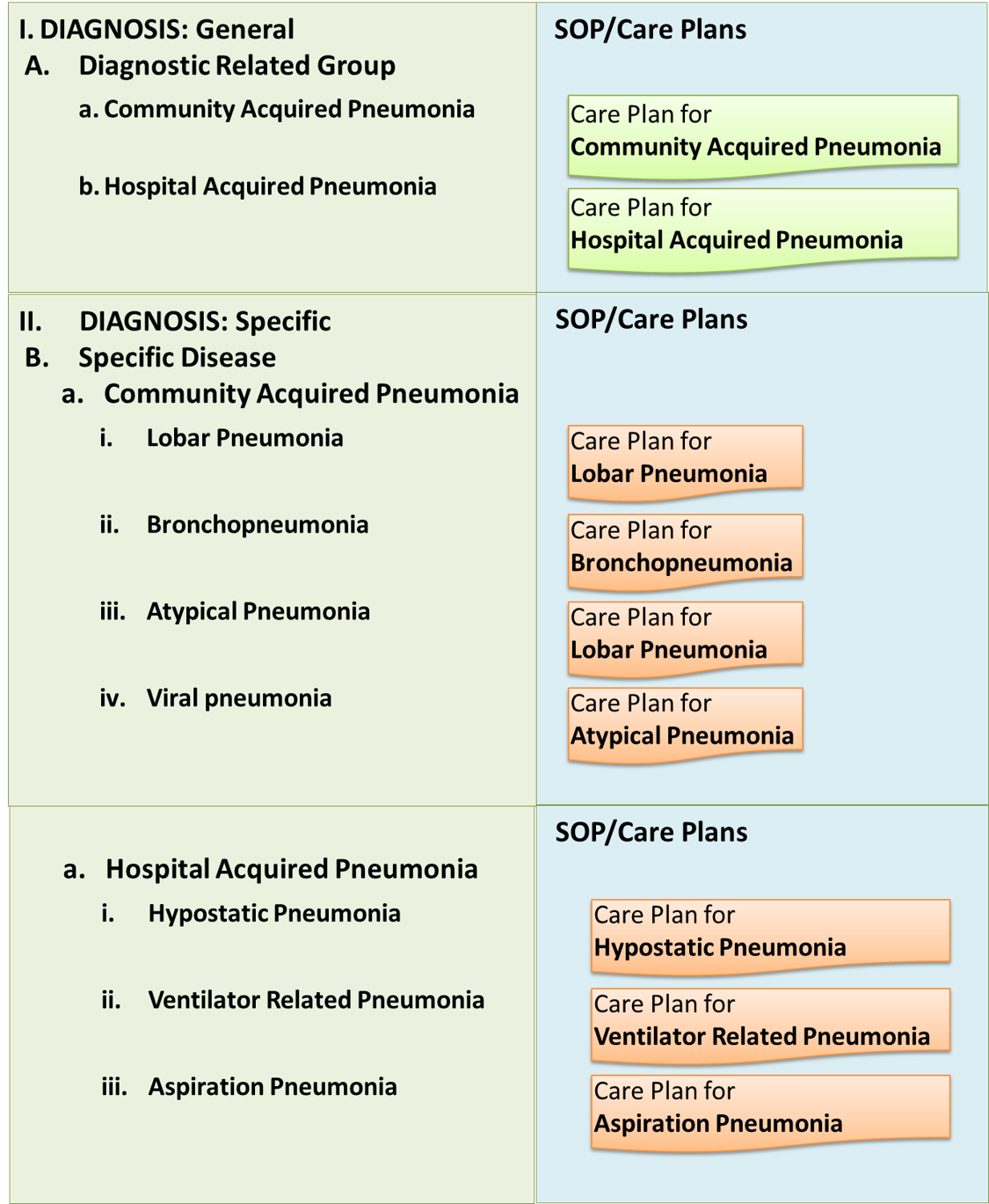
The effort of clarifying the diagnosis may yield a diagnosis that is a group of diseases rather than a distinct disease. For example, Pneumonia refers to a group of diseases characterized by infection of the lung consisting of Lobar pneumonia, Bronchopneumonia, Atypical pneumonia and variants related to the causative microorganism. As such Pneumonia is a diagnostic related group (DRG) rather than a specific disease. A SOP/Care plan has to be written for this DRG because it is important to provide the initial care of Pneumonia even when the cause is uncertain. When its variants are identified later, a specific SOP/Care Plans (based on causation) are required.
DESIGN FOR WHEN THE DIAGNOSIS IS CERTAIN
At the completion of the activities in the early phase of care, a definite diagnosis may be arrived at, and the patient profile is known. Then, an appropriate SOP/Care plan for the specific disease has to be developed.
The specific disease may be a typical disease or variants of it. It is necessary to make available SOP/Care plans for:
- main plan as applied to the typical disease
- sub-sets of plan for the category, stage, pathological grading, severity level, risk stratification and potential for remedy
- sub-sets of plan for alternatives, variations, options and contingencies
When the definite diagnosis of a specific disease is made with certainty, a SOP/Care Plan for the ‘care’ of this particular disease or health problem is used. The guidance given in it can be more certain, and specific. It will take a more didactic tone and be more regimented. The present illness is the primary consideration in formulating the service to be given to the patient (the service product).
| Working Diagnosis | Objectives | Care Plan |
|---|---|---|
| Specific Disease / Illness / Health Problem | Cure or Containment / Control or Palliation | Specific Care Plan – Initiate plan – Optimize care – Continue care |
CHANGE OF PLAN WITH FURTHER CHANGE IN DIAGNOSIS
Even if the definite diagnosis is considered to be certain , it may still change as the care process and the disease process proceeds because of additional information from developments that include:
- emergence of new symptoms and signs,
- physiologic changes evident by change in parameters monitored
- availability of investigation findings
- availability of data from better exposure e.g. findings at endoscopy or surgery
- observed changes in the response to treatment
As more clinical findings, investigations and monitoring data are available, a more specific diagnosis that is a refinement of the definite diagnosis or a complete change is possible. This warrants an alteration of the plan. If additional problems emerge, then there should be modifications to the plan.
If the change in diagnosis is minor then the same Reference plan is used but revised accordingly. If the diagnosis differs significantly, another more relevant Reference plan or sub-set of the previous plan must be chosen as a replacement. Hence, in designing the Reference Plan for a disease, besides making available a plan for a typical presentation of the disease, it is necessary also to build in advance appropriate plans for the variations of the disease.
Plans for Presumptive Working Diagnosis
There are instances when not all the criteria for a definite diagnosis are met, despite various efforts,. Then, either the provisional diagnosis or the closest diagnosis that can be reached (the Working diagnosis or Presumptive diagnosis) is used to select the SOP/Care Plan. The care provider must be aware constantly that this is the case and be ready to change the plan if further evidence points to a different diagnosis.
Retention of General Aspects and Refinement for Specific Diseases
The interventions within the SOP/Care Plans for Clinical syndromes and Diagnostic related groups are general. When the specific variety of disease is identified ultimately, the content interventions that are still pertinent are retained and further elaborated or can be discarded depending on their relevance. Hence, parts of the SOP/Care Plans that followed can be a continuation of the previous general plan but a significant portion will diversify along different paths.
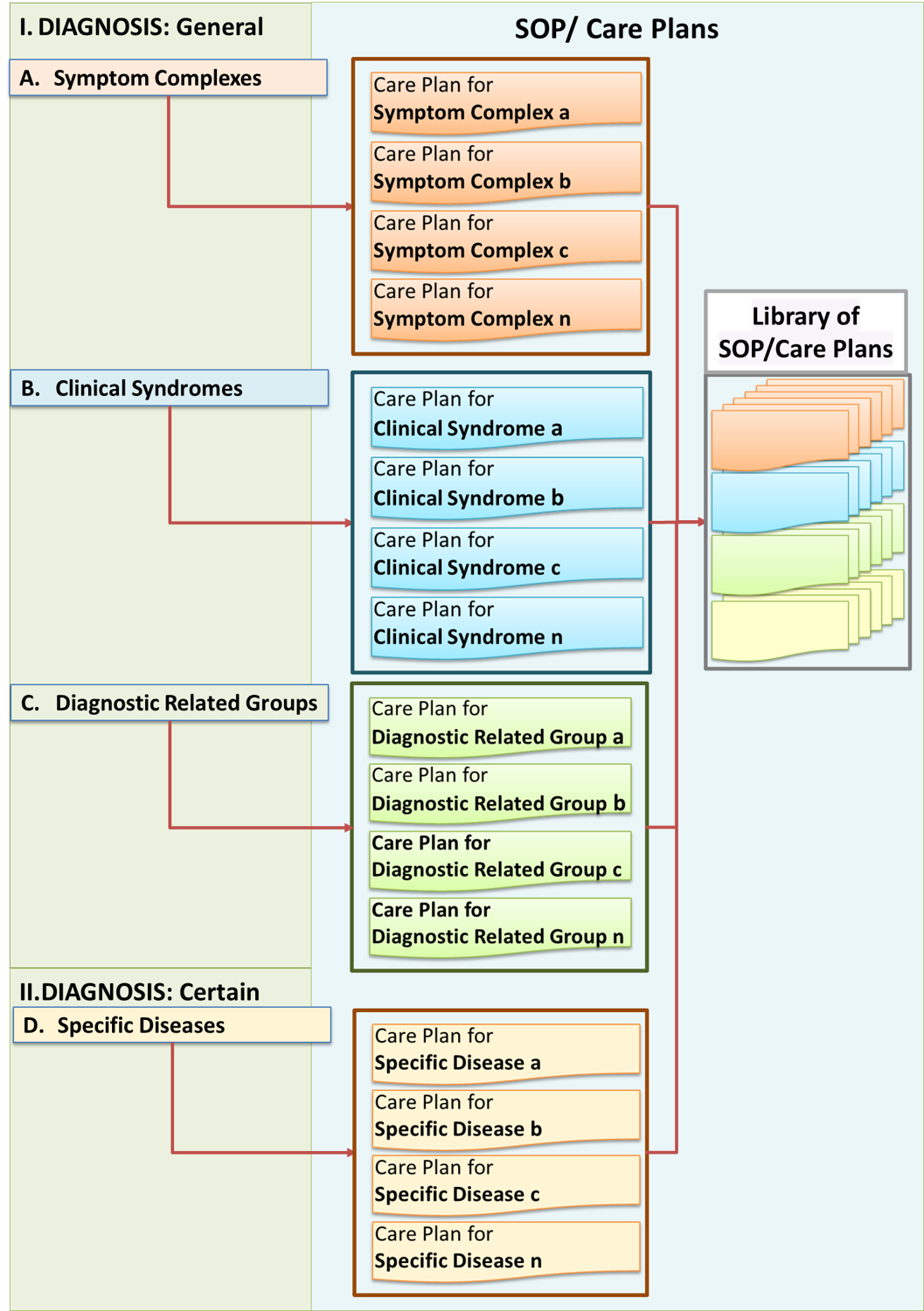
Creation of a Comprehensive Set of SOP/Care Plans
Plans for various diagnosis should be made available for reference (by whatever means) as a properly indexed comprehensive library of documents. In a paper based system, these documents are placed in files and compiled into folders usually termed as the Work Procedure Manual. In a computerized system, the documents are kept in a file server. They are systematically indexed and can be retrieved via a search mechanism.
Further Refinement of Care for Variations of a Disease
Even when a diagnosis is deemed to be definite (all the criteria to support it are satisfied), the care provider must identify the variant (sub-type) of the disease and the stage in its natural history. SOP/Care plans must be designed not only for specific diseases but also their variants. Diseases can be stratified according to categorization, staging, pathological grading, severity level and risk stratification. These variations must be considered when SOP/Care plans are designed and chosen.
Types of variants of diseases include:
- Pathological variant
- pathological grade, (virulence of causative organisms, tumour cell type, degree of differentiation of neoplasms)
- clinical onset (acute, chronic)
- Clinical variant
- the stage at time of presentation relative to its natural history (early, late, presence of complications)
- severity level (mild, moderate, severe)
- Patient profile / category
- age,
- gender,
- risk factors,
- confounding factors.
The above variations will impact on both the way the case is cared for and the expected or desired outcome. Where disease variants are known, plans for its care can be written as extensions or appendices to this SOP/Care Plan of the disease. Where the alternatives are subtle, variance to the SOP/Care Plan can be made by the clinician him/herself when devising the Actual care plan.
Where there are very distinct variations, the care of these sub-types can be considered as essentially different service products. A separate sub-set of the SOP/Care Plan should be created for each one of the sub-types.
Plans In Response To Variations, Options and Contingencies
At the start of care (usually at the first session) the primary provider chooses a care plan that matches the diagnosis. At subsequent sessions the same plan may be used if appropriate. There will be a need to design a sub-set of the plan depending on variations in the pathological grade of the disease, the stage of the disease, the level of severity or the emergence of complications.
Indeed, a Reference Care Plan for a different disease must be available for the clinician when there is a marked change in the diagnosis.
Plans are also modified or revised if various other emerging needs appear. If formally designed plans are not available, then the care provider needs to devise the actual plans him/herself without referring to a Reference plan. Hence, it is better to design and put together a comprehensive library of Reference Care Plans to cater for various scenarios in the care of a patient for each disease, illness or health problem. The primary provider selects the appropriate plan from a library of SOP/Care Plans made available to him/her.
STEP2: Setting the Standards for the Expected or Desired Outcome
Standards for the expected or desired outcome are condensed from the the objectives of the service. Broadly, the care objectives (expected outcome) are:
- Cure
- Containment (by 2O or 3O Prevention)
- Palliation
Which objective is suitable depends on the diagnosis and therefore the service product.
Note: Standards for input (facility, machines, human resource etc.) are mentioned as policies when the procedures are described.
Objectives of the Service and Standards of the Product
The primary objective of any service is satisfying the needs of the client and the product is said to be “fit for use”. In patient care, a good service is defined by a set of prominent features or characteristics i.e.:
- effectiveness
- safety
- acceptability
- appropriateness
However, besides these main features, attention must be given to secondary and tertiary needs of the patient including:
- accessibility,
- convenience,
- responsiveness,
- affordability,
- comfort
At the same time, attention should be paid to the viability of the service as a business venture. It is necessary to take into account efforts directed towards ensuring:
- feasibility
- productivity
- efficiency
- cost-effectiveness.
- lowering of risks.
Many of these characteristics are interdependent. Acceptability depends very much on affordability, convenience, comfort and timeliness besides conformance with cultural values. In turn both timeliness and affordability are the result of efficient service delivery. Feasibility depends substantially on capability (availability of resources) and cost-effectiveness.
The general objectives of the service are used to guide the development of and therefore built into every aspect of the service. In the SOP, it is not necessary to document them as a separate section except perhaps to mention them in the introduction.
Objectives and Standards of the Care of a Specific Case
The objectives or outcome goals of the service provided (i.e. care of the patient) should be known and stated at the outset in the SOP/Care Plan. Of course this depends on service product which in turn depends on the diagnosis. In fact, objectives are determined for every phase of patient care and for every intervention made.
At the early phase of the care episode when the diagnosis is yet uncertain the care objectives would be achieving adequacy in:
- relief of symptoms
- provision of support (physiological, psycho-social)
At the later phases when the diagnosis becomes more certain and more definitive treatment is given, the objectives can be more definite. The final objective or treatment end points need to be defined and measurements made to determine whether they have been achieved. Depending on the disease, the objective of treatment would be the combination of any of the following:
- cure the illness,
- contain it or control the progress and minimize complications
- mitigate the effects
The objectives of care influence the way it is planned. For a given illness, not all of the objectives mentioned can be achieved or are necessary. While many diseases are eminently curable, some can only be contained or their harmful effects reduced/mitigated/delayed. When there is potential for cure or complete resolution of the disease process, the plan is directed towards achieving it. In such illnesses achievement of the objectives is the marker for ending the care episode.
Even as attempts are made to achieve cure, efforts must be made to at relieve of symptoms, contain of the effects of the disease through physiological plus psycho-social support and rehabilitation. Therefore in a patient where cure is possible, the therapeutic (treatment) approaches or modalities will have the following intentions:
- Definitive
- Symptomatic
- Supportive
- Preventive
- Rehabilitative
- Promotive
For patients with diseases that are inherently incurable or are too far advanced, the plan offers beneficial therapeutic options aimed at symptom relief, restoring functions, and providing comfort. This mode of therapy is termed as Palliative care. Achievement of the objectives mark the point when the care is considered to have been optimized.
Whether the intermediate or final objectives are achieved is estimated and decided at the procedure of Progress Review. The progress of the patient is a measure of outcome. The criteria is the detection of deterioration or improvement and occurrence of complications of illness or of treatment.
Standards of the Outcome of Care
Standards are quantifiable characteristics that form the relevant criteria based on which the achievement of the objectives are determined. The criterion can be a measurable value or if subjective its value is being present or absent. Often the outcome is computed from a set of characteristics or parameters with each characteristic given a nominal value or score. The parameters can be clinical symptoms and signs, physiological status, biochemical measures etc. This method of measuring outcome is termed as a “scoring system”. The most important standard to be declared is that of the intended or expected outcome with respect to the illness..
Prognosis
The likelihood that the above outcomes can be can be achieved is termed as the “prognosis”. It is based on the analysis of results from a study of a population of similar cases. Since outcome is dependent on severity of illness, the presence of of factors contributing to the severity can be assessed at presentation and summated as a scoring system. Comparison of the final outcome of a case with prognosis (expected outcome) for similar cases similar in severity is a better measure of success.
STEP 3: Putting in Place the Service Delivery System
Standards for input (facility, machines, human resource etc.) are mentioned as policies when the procedures are described.
For any service to be offered, the organization/facility has to ensure that a proper service delivery system is in place. When a new facility is built the input required to deliver all of its service products must be built or procured. If a new service product is to be introduced in an existing organization, then whatever additional facility, equipment and personnel require must be made available.
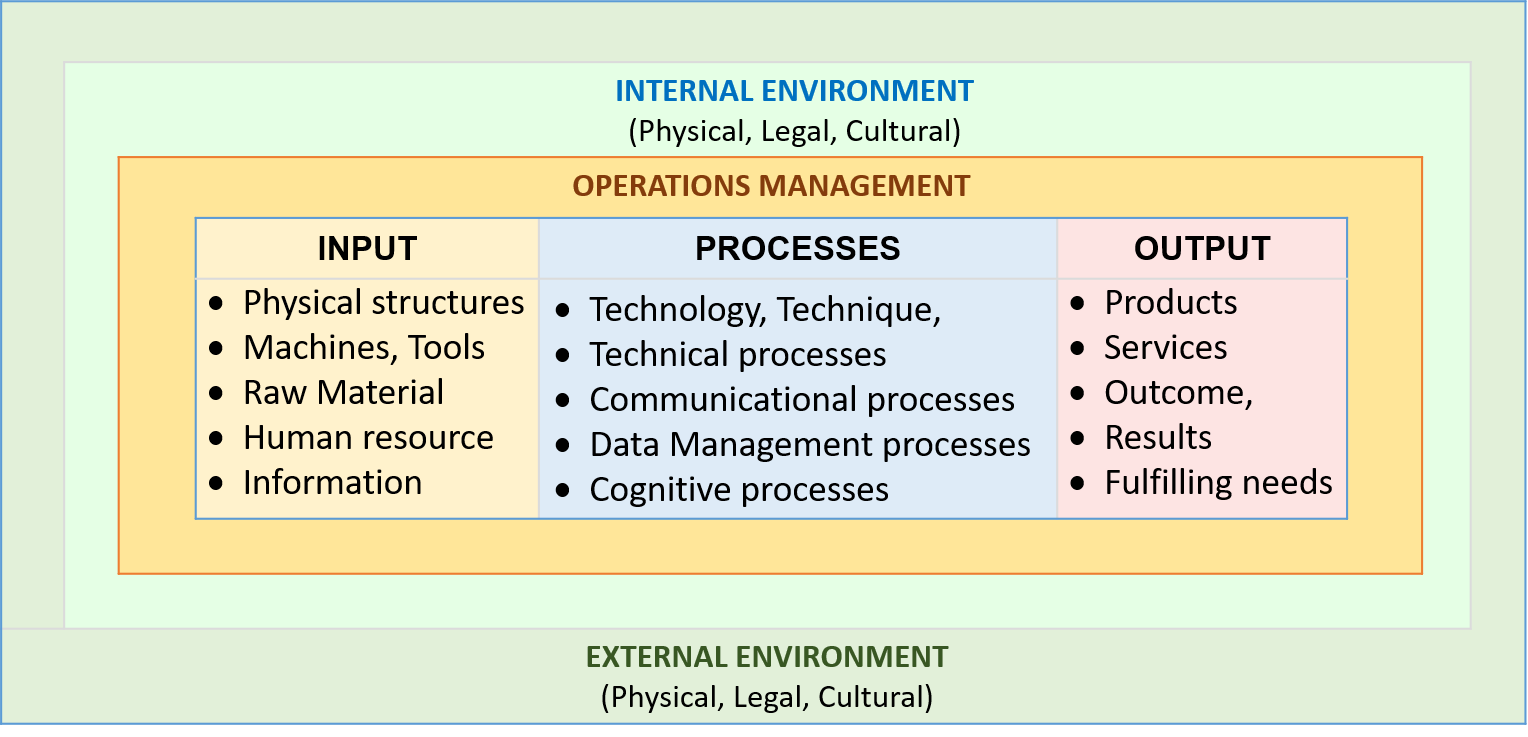
The factors that impact of the operations of a patient care service is illustrated below:

Location
Each service product must be delivered at appropriate locations. The choice of the location depends on the sessions to be conducted, types of procedures to be performed and the needs of the patient. Each location is a service delivery unit with specific settings i.e. the facility design (layout) and the resources made available and accessibility. The types of service delivery systems include:
- Outpatient clinic
- Emergency complex
- Inpatient ward
- Day Care complex
- Procedure rooms (for surgery, endoscopy, tests etc.)
- Home
- Teleconsultation facility
The complexes or units have general requirements of and follow certain systems. These are known and can be assumed to be in place. However, if specific requirements and specifications are required this should be stated in the SOP/Care Plan at the beginning or mentioned as and when the procedures are described.
The choice of service delivery systems in relation to sessions (visit, events) can be proposed as a general rule but often can be made at the actual implementation of the plan. This will be discussed later in the appropriate sections.
Staffing
Standards of Input
Lists given as attachments. Standards for input (facility, machines, human resource etc.) are mentioned as policies when the procedures are described.
STEP 4: Design and Composition of the Method of Delivery of the Service Product
Just as various methods are used to manufacture tangible products, suitable methods are devised to deliver service products.
Delineating the sequence and layout of the workflow (the Care Pathway, the phases of care))
Providing clear instructions on the policies and procedures to follow (legal, professional and ethical considerations)
Identifying the most appropriate technology or modalities to be used
Assignment of responsibilities to various service providers
Identifying the monitoring and control measures (Monitoring, Review and Evaluation, Quality Control)
Providing reference documents (work instructions, standards)
Providing the means for data documentation (Clinical documentation, Forms, Charts, Information systems)
Anticipating possible errors of omission or commission, their prevention and damage control (Quality control).
providing alternative actions to cater for variations, exceptions and contingencies.
- Procedures (Clinical Care Processes, Workflow, Care pathway)
- Information gathering
- Deriving conclusions
- Planning
- Execution
- Review/Evaluation (of diagnosis, objectives and plan)
The Delivery of Clinical Patient Care Service
Work and Services
Work is the expenditure of energy to produce a useful outcome. It is made up of a series of activities performed by workers. Each activity consists of a series of procedures or tasks. Therefore, patient care service delivery is the performance of various activities to improve the condition of a person affected by an illness, disease or health problem.
Policies and Procedures
The principal purpose of the SOP/Care Plan is to indicate the set of procedures required to conduct the care of a patient. Policies provide the limits or constraints within which procedures are performed. Hence, the development of effective SOP/Care Plans requires a thorough understanding of the clinical work processes and the policies that govern it.
In healthcare, the word procedure is often used differently to mean some intervention done directly on the patient like a surgical operation, endoscopy, taking blood and so on. In this discussion, the term procedure is taken to mean, just as in other industries, a group of processes performed together to produce a certain output or outcome. To avoid ambiguity, the term task is taken to be equivalent to this meaning of procedure and is preferred in this discussion.
General Policies
General policies are rules that take into consideration the values held by the facility or organization where the service is provided. They may include:
- philosophy, aspirations, goals and principles of the facility or organization
- adherence to legal requirements
- conformance to professional standards
- ethical considerations
General policies of the facility/organization should be indicated in in its business plan. However general policies must also be written for every service product.
Legal and Ethical Considerations
Patient care is a highly regulated service. The design of the SOP must take into account legal and ethical requirements including:
- ensuring privacy
- maintaining confidentiality
- showing respect for human dignity
- obtaining consent
- use of accepted methods and technology
- performance of tasks only by qualified persons
- use of properly functioning and safe equipment
- providing the service in a safe environment
Legal requirements vary from country to country. Ethical norms are advocated by professional bodies (councils and associations). These requirements must be stated as general and operational policies in the SOP/Care Plan.
Operational Policies
Operational policies are guides on how to perform procedures and achieve the expected results. They are molded by the general policies and then constructed around the procedures used to deliver the service product. They define limits and constraints on what must be done, what conditions must be satisfied before it can be done and what to avoid. They are embedded within the procedures.
Policies Aimed at Achieving the Objectives Of Care
Striving to achieve the objectives of care is itself a policy. It is often termed as the Quality policy. Hence, the care provider must be aware of the desired outcome at every step of the care process and use it as a guide.
Procedures (Tasks)
In other industries, the term procedure is taken to mean, a group of processes performed together to produce a certain output or outcome. In healthcare, the word procedure is often used differently to mean some intervention done directly on the patient like a surgical operation, endoscopy, taking blood and so on. To avoid ambiguity, the term task is taken to be equivalent to this meaning of procedure and is preferred in this discussion.
| Term | Meaning |
|---|---|
| work | the expenditure of energy to realize a useful outcome |
| workflow | the sequence and direction of how work is done |
| processes | the most elementary unit of work |
| procedure | a series of processes |
| tasks | the alternative term in healthcare for procedures |
| product | the useful outcome (object or benefit) achieved through work |
| service | an instance of providing a benefit to a customer |
| care | alternative term for service provision in healthcare |
| healthcare | the service of promoting, preventing, maintaining and restoring health |
| delivery | provision of services, an alternative term for operations |
Performance of Tasks
In patient care, tasks are performed by workers delivering services who are called care providers. A service is made up of a series of planned tasks and their delivery. The instructions or requests to perform tasks are called orders. Work can be done in many ways including:
- manually by the care provider or a team of care providers
- by the care provider with the help of machines.
- by a machine based on instructions given by a worker and under his/her supervision
- entirely (automatically) by a machine prompted by instructions built in computer applications
As part of the service, items such as drugs, blood products, fluid and nourishment are given or supplied to patients. These tasks must be done in an accepted way. They are often called dispensing or administration.
Procedures as a Series of Processes
Tasks are made up of processes. In caring for a patient, healthcare professionals act as a team. They are dependent on the contributions provided by each another.
In patient care services, tasks are performed in many ways, using various input. Many are technical i.e. performed manually or with the help of machines which can be automated. Some take the form thinking (cognitive) processes but most are a mix of both types of processes. Some of the most common processes is that of data management.
Because functions are performed by persons with the ability to perform them, tasks are allocated to a particular professional or teams of professional. Many procedures can be accomplished only by a team of personnel.

A task should be performed only by a worker with the skill and knowledge to perform it. Even then, he/she must do so using the right input and within a suitable environment. Input includes items such as raw material, instruments, assistance and information. In fact, the ability to proceed from one task to the next depends on whether the results of the transformation made by the previous task is immediately available and sufficient. If so, he/she may continue to the next task without pause. Therefore, an essential input is data (results) generated by the previous task.
The environment suitable for a task takes into consideration situations such as the adequacy of space, cleanliness, air quality, safety, lighting, noise level, presence of essential equipment and proximity to other facilities.
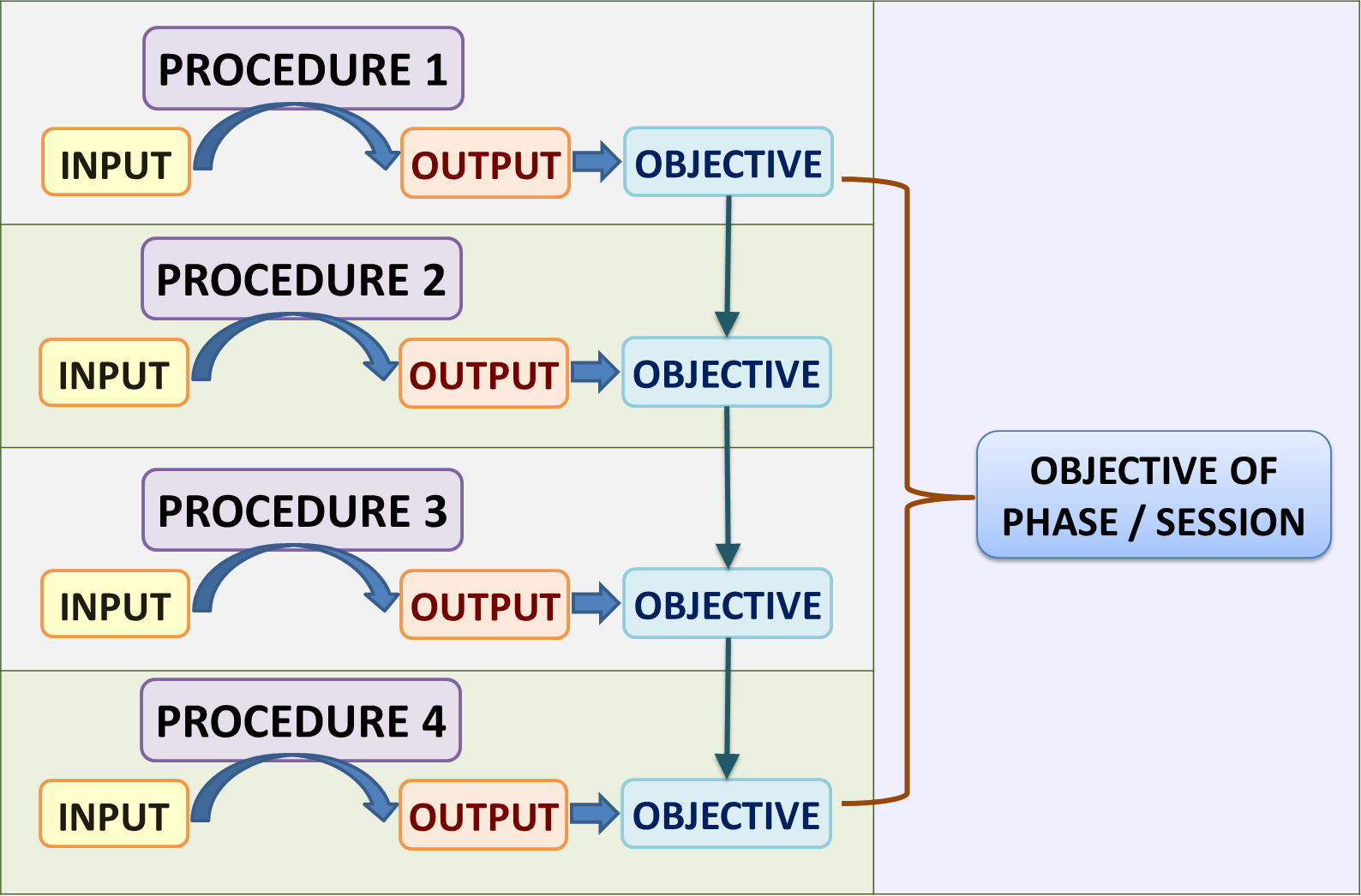
Output and Objective of Procedures / Tasks
Clinical care is made up of procedures each of which produces outcomes that contribute to the fulfillment of the objectives of care. Procedures are considered successful if satisfactory results are obtained. Otherwise they be repeated or replaced by another method. The whole care episode is divided into phases and sessions within which sets of procedures are planned with the aim of achieving various objectives which when added up will lead to the desired overall or final outcome.
Sequence and Direction of Procedures: The Workflow
The predicted or planned sequence and direction and layout of what, when and how work processes are to be done is termed as the ‘workflow’. It is the practical application of the sequence and paths thought out through algorithms. In manufacturing and most service industries the techniques used are capable of producing precise results. Therefore, procedures are performed in fairly fixed sequential steps.
In patient care, the sequence is less rigid or predictable. Actions at subsequent steps are often dependent on the outcome of the previous steps. Hence, procedures are often cyclical or iterative.
There is a universally accepted way by which clinical care providers deliver patient care. The services consist of two categories:
- Administrative tasks
- Clinical tasks
Administrative tasks are those tasks that facilitate the management of the patient as a client which include giving appointments, registration, admission, resource allocation,referrals, transfer and discharge, and follow up. They contain processes different from clinical care processes and require separate SOPs. They occur at the beginning or end of the service and sometimes interspersed between the clinical tasks. In the clinical care process, they should be mentioned but need not be described in detail.
The path/flow/sequence/layout of processes is thought out and later presented in two ways i.e.:
Outline of the Workflow
A general outline of the workflow is often called the high level workflow or ‘critical’ pathway. It contains only the critical (important, required) steps) with the obvious or mundane steps left out in the documentation (but not in practice). When the processes are complex it is beneficial for better understanding to demonstrate the flow initially in the form of an outline and details are elaborated subsequently. The outline of the generic flow of clinical care is as shown below:
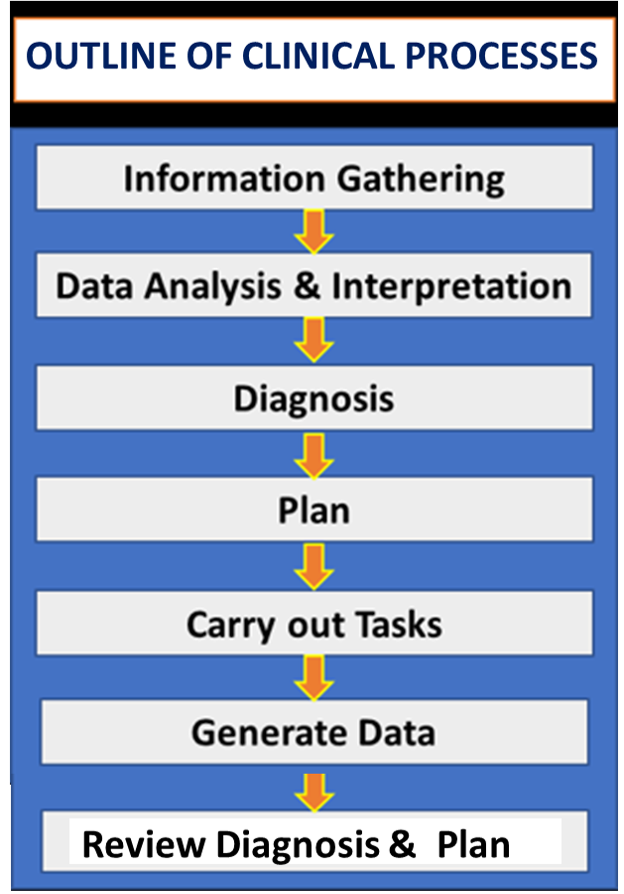
This general workflow is applicable to most cases. However the sequence of the processes does not necessarily follow this strictly but will depend very much on the type, severity, urgency, speed of progress and effects of the illness. In an urgent case, emergency treatment is given first before a full interview, examination and tests are done. Some cases may have obvious diagnosis based on routine tests or chance findings from investigations already done during other instances of care. As such, it would not be necessary to repeat the diagnostic investigations. For some types of cases, it may be more practical to perform certain processes first as a routine for example performing urine tests at a antenatal visit or visual acuity measurements for every case with a problem of vision.
In some instances the following scenarios that affect workflow can occur:
- results of tasks are available or become evident only after an interval,
- the next transformation must be performed performed by another worker.
For the first scenario, the care provider has to stop, wait for the results and resume his/her work when they are ready. For the second scenario he/she has to pass on the next task to another worker. He/she may resume his/her part of the work when the transformation has occurred or the results are ready.
The workflow has decision making steps i.e. points when care providers have to choose the appropriate path when alternative directions exist. The decision is guided by criteria such as:
- policies,
- judgement,
- patient preference,
- availability of resources.
Working Out a Detailed Workflow
There is a universally accepted way by which clinical care providers deliver patient care. The services consist of two categories:
The path/flow/sequence/layout of processes is thought out and later presented in two ways i.e.:
- written as a narrative,
- depicted graphically as a chart
The workflow is first thought of as a series of steps consisting of the arrangement of the tasks for the delivery of a service in terms of content, layout, sequence and direction. The operational policies are embedded within it. The set of procedures and their sequence is outlined below:
- G
eneration, gathering and collection of data about the patient’s illness and the effect on his/her health through interview, examination, observation, measurement, tests and investigations by various techniques, - Documentation of data regarding tasks done and their results plus reporting incidents that happen and the actions taken (using specific forms and charts).
- Analysis and interpretation of data to determine the diagnosis, status, profile and needs of patients,
- Planning the case management including response to anticipated side effects,
- Therapeutic tasks (treatment, providing support, rehabilitation, preventive actions, damage control) using various modalities.
- Monitoring and Progress review
- Continuation or discontinuation of the care depending on the outcome.
Each of these steps will be discussed in detail
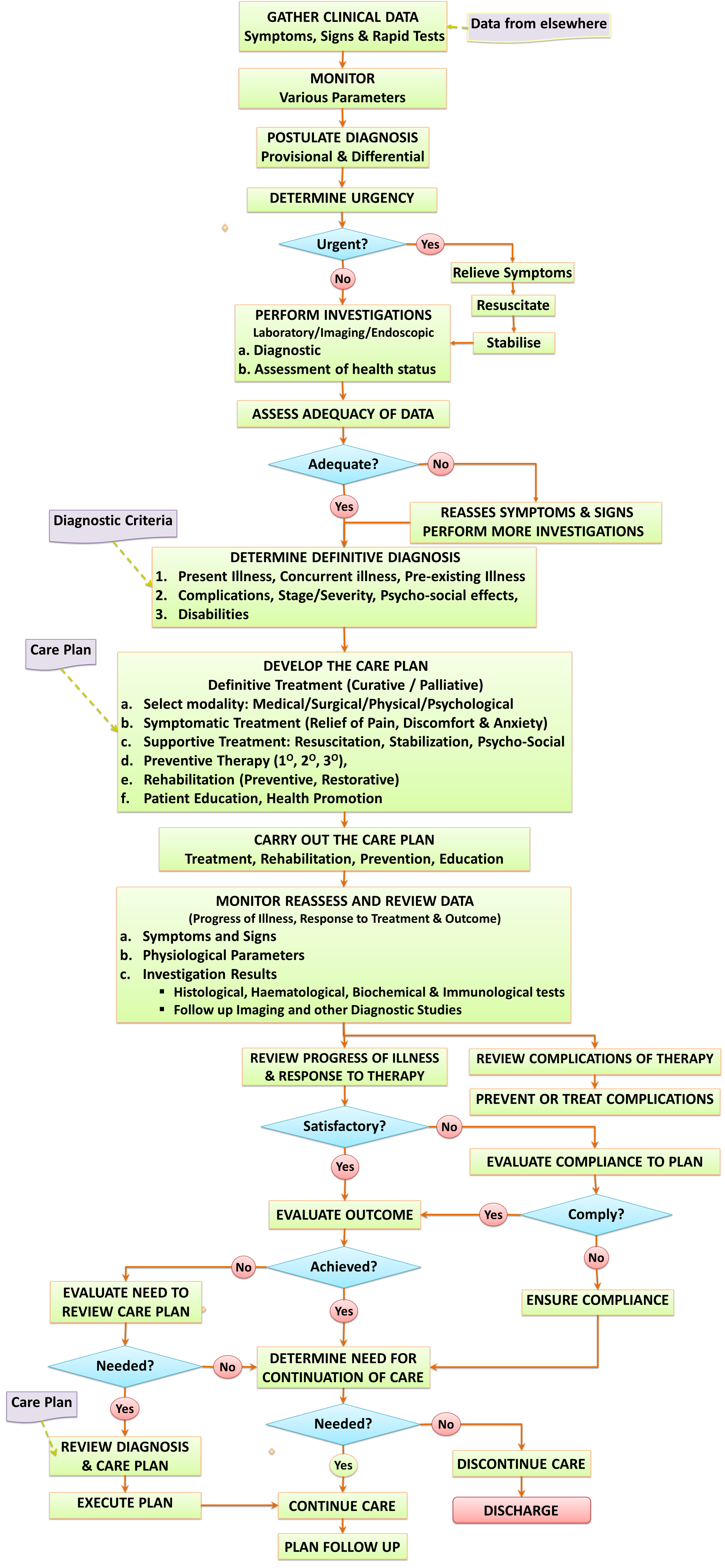
Graphical Depiction of the Flow Of The Clinical Process
In the SOP/Care Plan, the understanding of the flow, sequence and layout of clinical processes is much enhanced if depicted graphically as a workflow chart. However, it must always be preceded or followed by a narrative description. The workflow that can be applied generically for patient care is as depicted below:
Decision Making Steps an Essential Component of the Workflow
Decision making steps is an essential component of the workflow because its determine the direction of the steps of the care process.
In clinical care, the plan is very much dependent on diagnosis. After selecting a plan based on the initial diagnosis, the care provider may decide to alter or revise the plan based on the criteria listed below:
Changes in the understanding of the illness affecting the patient (the certainty and comprehensiveness of the diagnosis )- Evolution of the disease along its natural history,
- Advancement of the flow of clinical processes,
Occurrence of other emerging issues (incidents, contingencies)
There are instances when the workflow cannot progress according to the initial plan due to various impediments or circumstances. At times, the processes e.g. information gathering, investigations or tasks have to be repeated or abandoned. In those cases or if the prescribed treatment plan is ineffective, unacceptable or unsafe for the patient, an alternative approach or modality is used. Non-compliance by care providers or patients is also a factor that affects the progress of the workflow as well as the success in achieving the desired outcome.
Decision-Making and the Resultant Change in Plan
- Guide to making decisions
- Indications,
- Contraindications,
- Precautions (preventive measures, risk control)
Decisions are made when there are choices or options to be selected. In clinical care, decisions are made based on conclusions arrived after appraising the situation based on accumulated information. The conclusion may be determined by appraisal of:
- the updated working diagnosis
- the latest understanding of the disease/problem,
- the evolving objectives of care,
- the progress of the disease,
- the response to treatment.
The choices or options that a care provider can make are:
- to retain the current plan without alteration,
- to make modifications to the current plan,
- to change the plan completely to a new plan.
SEQUENTIAL VS SIMULTANEOUS TASKS
Whether tasks are performed sequentially or simultaneously need to be addressed in SOP/Care Plans. Tasks need to be sequential if it requires:
- active involvement of the patient
- the use of the result of another task.
The involvement of clinicians are often through direct interaction with the patient. When the tasks requires the patient to cooperate by physical or verbal means, care providers have to take turns to perform them. This is because a patient can only be at one place or interact with one care provider at one time. Only when the patient is free another clinician may use the opportunity to have direct contact whether to gather information or provide direct care. For example, after the doctor has done his /her round, nurses do their own to observe, monitor and chart various parameters .There are exceptions to this rule like when active input from the patient is not required, tasks can be done simultaneously by different care providers. For example, a nurse may observe the patient while the doctor is talking with or examining him/her. There are instances e.g. in emergency situations and in complex procedures (e.g. surgical operations) when more than one care provider may be attending to the patient at the same time. Often, when the patient is unconscious (comatose or under anesthesia) different interventions are done on him/her.
Tasks that does not require the presence of the patient can be done simultaneously or concurrently. Hence, tasks such as making a diagnosis and planning can be done while another care provider is attending to the patient. These are thinking tasks that uses data from memory or from records. Sometimes, the ability to perform it requires the presence of the medical record. In computerized systems data can be presented as views or displays.
Procedures performed in the presence of the patient must be performed sequentially.. These include those performed by Radiologists, radiographers, echocardiogram technicians, endoscopists, optometrists, and audiologists.
Pathologists and microbiologists usually work on specimens obtained from the patient and therefore their tasks can be performed concurrently in parallel with that of clinicians.
REPETITION AND ITERATION
In the manufacturing industry, tasks are usually done only once. Repetition is called rework and seen as a failure. The same is true for most clinical tasks. The dictum “do it right the first time and every time” is also applicable to clinical patient care
However, cycles of events and tasks are often repeated not because they fail but intentionally. for various reasons. This repetition of cycles of events and tasks is termed as iterations
Meaning of Iteration: repetition of a sequence of operations that yields results successively closer to a desired result.
Repetition of Procedures
During the entire episode of the care of a patient, the procedures of interview, examination, tests, diagnosis, plan and evaluation often forms a repeating cycle.
Therefore, care is fashioned in blocks within which there are iterations of various events and tasks. This is because the objectives of a care episode is achieved through the summation of objectives of the various phases. For each phase, the objectives are rarely achieved by one cycle of processes. In most cases, the objectives can be met only through a series of purposeful repetitions. Only by the achievement of objectives of a phase would care be able to move on from that phase to the next culminating in the final outcome.
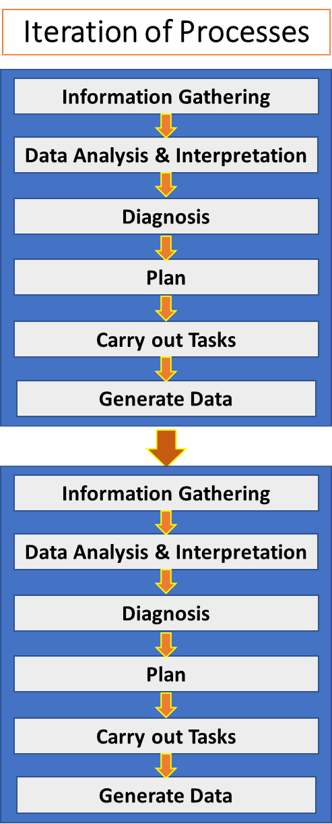
The repetition of the clinical care processes makes the work cyclical. Each cycle is termed as an iteration and clinical care is said to be iterative in nature.
Purpose of Iterations
Iterations are necessary because clinical patient care mirrors the steps of data management which is made up of:
- gathering data,
- putting them together,
- analyzing them,
- interpreting them,
- deriving conclusions based on them, and
- acting on those conclusions.
Actions will generate more data which must be managed according to those similar steps. Results of analysis, interpretation, conclusions and actions becomes new data.
Furthermore at some parts of the care episode, some work may have to be repeated until satisfactory outcomes or results are obtained. Repetition is required in circumstances when:
- the work is effective only if it is repeated intentionally for a certain number of times
- failure to obtained satisfactory result by a single instance
- the work has not been carried out properly
- the patient’s condition changes as the disease progresses naturally or because of treatment. Repetition of monitoring of parameters, tests, progress review and measurement of outcome will provide data that will show the trend,
Benefits of Iterations
Iterations are beneficial because it enables the clinician to:
- obtain more data of increasing range (granularity) and accuracy and complete the data management cycle
- reach a more certain and comprehensive diagnosis
- demonstrate the status of progress of the disease and patient’s condition
- ascertain the effectiveness of treatment
Iteration As the Means to Improve
Iteration of the processes of data gathering, collation, analysis, and interpretation is necessary to make data more accurate, and sufficient. Interview and physical examination is repeated to determine progress of existing symptoms and signs or the emergence of new ones. Investigations are redone if there are problems with the sample or the test itself. They are repeated to see trends in the results.
Because data acts as input for the formulation of diagnosis, the increasing amount and quality of data obtained from each cycle will facilitate the derivation of increasingly more accurate and comprehensive diagnosis as care progresses. Monitoring and review are necessarily iterative tasks.The recommended treatment regimen should be provided in the reference SOP/Care Plan. However, often when implementing the actual plan, to achieve the optimal result, therapeutic measures such as medication, irradiation, or physical manipulation must be improved by altering the dose, intensity, technique, or frequency.
While surgical procedures that causes permanent change cannot be repeated others that result in temporary benefits (such as dilatation, debridement) may be repeated. As a rule, treatment as an event undergoes first iteration of the tasks of plan, initiate, review (iteration), followed by subsequent iterations consisting of modify, plan, implement and review again.
he increasing clarity and validity of data, diagnosis, and plan means that the service is constantly undergoing quality improvement. This feature is quite unique to clinical patient care.
From the above discussion, it can be seen that an important reason why iteration is necessary is the need for increasing quantity and quality of information. In that respect, iteration can be seen as the repetition of the data management cycle as shown below:
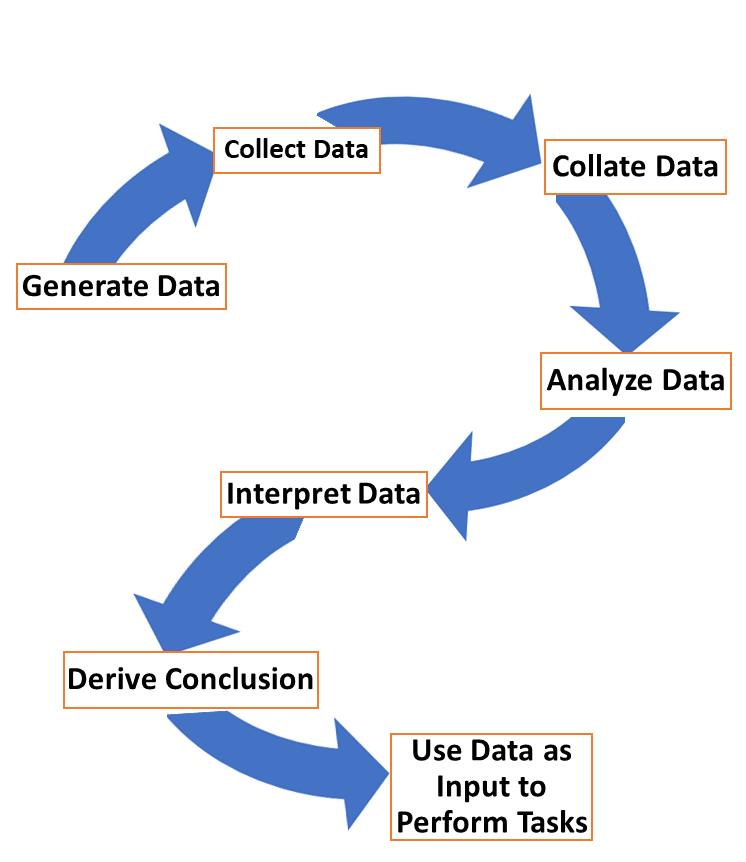
Data made available after an iteration of a data management cycle becomes an essential input for all clinical events and therefore drives the clinical workflow.
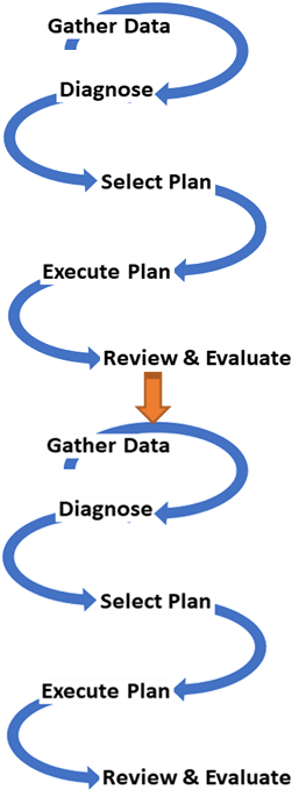
Steps in Fabricating a Product or Realizing the Outcome
In any manufacturing industry, producing the output is achieved through many separate activities. that usually include processing of the raw material, fabrication of parts, assembly, testing and distribution. The activities are usually in sequence but parts may be built separately before being assembled. For some of the activities, the processes are strictly continuous e.g. in an assembly line, but in others these c an performed with intervals in between and done at different facilities.
Services in healthcare are delivered in a similar way. The entire Care Episode is considered as as a package of services provided in stages. Each stage consists of sets or blocks of activities.
The Care Episode
In a patient’s lifetime, he or she may experience multiple illnesses, diseases or health problems. The entire period during which care is delivered for one of them is termed as the Care episode, It mirrors the disease episode. It begins at the time of first contact with a health care practitioner and ends, in most cases, with the resolution of the illness/problem or death of the patient. It is necessary to view the care episode from separate angles:
- the period during which the service product is delivered
- the scope and content of the SOP/Care Plan for the service product
Besides what is delivered to the patient, what he/she experiences during the care episode is also the service product. The SOP/Care Plan confines itself only on how the service is delivered.
Dividing the Care Episode into Phases
The care episode advances in sequential major steps over time. These steps can be termed as phases. Each phase is made up of blocks of procedures carried out to attain an intermediate objective. The final outcome of care is achieved through the fulfillment of objectives of each phase. The phases have variable number of procedures and take variable duration to complete.
The phases of care of both acute and also chronic diseases are categorized and sequenced based on their functions as listed below:
- establishing diagnosis, stabilization and immediate care
- initiation and optimization of care
- maintenance of care, re-evaluation and modification
- discontinuation of care in the event of resolution of illness
Blocks of Activities within a Phase
The activities within each phase of care are iterations of the processes of care. Hence the plan for each phase consists of procedures sequenced according to the flow of the clinical care processes. The differences between the phases are in the
- aim i.e. what should be achieved at that particular point
- focus i.e. what measures should be emphasized on.

In the SOP/Care plan document, this complexity can be clarified by dividing the description of care into different sections and paragraphs differentiated by headings.
Progressing through the Phases
The plan of care moves from one phase to the next depending on the increasing certainty and accuracy of the diagnosis. The care given does not wait for when a definite diagnosis is available.
Therefore, plans must be available for care when the diagnosis is uncertain (symptom complex, clinical syndrome) as well as when the diagnosis is certain (disease group, specific group and variants of the disease). The clinician need to select and use the care plan appropriate for the working diagnosis as the care progresses through the phases. How Reference plans are combined to form the Actual Plan of care will be discussed in detail later.
Activities within a Phase
Within a phase, the ability to perform each task is dependent on the outcome of the previous task. Therefore as a rule, it is important to perform the set of tasks in sequence.
However, this sequence may not be strictly followed because there are times when:
- an opportunity to perform the task may not occur again,
- it is more convenient to perform an activity earlier or later,
- one activity may be given priority over another because of certain needs.
When designing the SOP/Care Plan, it is necessary to think out and list down the whole series of tasks within the care episode. It may be appropriate to depict them as a single list of tasks in the Reference Plan but as will be discussed later, in the Actual Plan the tasks have to be divided into sets or blocks of tasks so that they can be allocated time slots and assigned to particular care providers. At the time of designing the Reference SOP/Care Plan, the separation into discrete blocks is not possible because of the following reasons:
- in patient care, an activity need not be carried out at the same location or facility,
- alternative equipment may be used to perform certain tasks,
- the ability to perform a task is not necessarily confined to a particular care provider category,
- often there is a need to repeat the tasks before the desired outcome is achieved, The frequency of this repetition is not predictable.
- clinical tasks of data gathering, diagnose, plan, treat, monit
- or and reevaluate take a variable amount of time to complete.
- the advancement of the care process is related to how the disease progresses which is not always the same,
- the response to treatment is not uniformly predictable.
Dividing Care into Sequential Phases
As discussed earlier the planning of care occurs continuously throughout the entire episode of care. The care episode is divided into sequential phases during which groups of procedures are performed aimed at achieving distinct purposes or objectives. So, a phase starts with the setting up of one or more objectives and ends when all the objectives have been met. This occurs when all the tasks designed to achieve the objective are performed successfully. Completing all the phases will then result in the final outcome. Hence, the phases and the care episode are not limited by time or number of sessions (will be discussed in detail later).
The Plan for Each Phase
The care episode can be roughly divided into two periods i.e., the phase when the diagnosis is being formulated and the period consisting of the phases after a definitive diagnosis is made. Actions taken at the earliest phase is concerned mainly with establishing the diagnosis, stabilization of physiological functions and immediate care. At the end of this phase the definitive diagnosis should be obtained. In the next phase, attention is given to starting the definitive care and optimizing its outcome. This is followed by efforts at continuation or maintenance of treatment, monitoring and reassessment. Subsequent actions depend on whether the illness resolves such that care can be terminated or remain unresolved hence requiring continued care.
The phases of care of both acute and also chronic diseases are categorized and sequenced based on their functions. They can be given different names but the following division is typical:
- Phase of determining the diagnosis and immediate care / early treatment
- Phase of initiation of definitive care
- Phase of optimization of care
- Phase of maintenance of care
- Phase of resolution (continuation or discontinuation of care)
Procedures within Each Phase
Despite this division the activities within them are contiguous. However, because of the iterative nature of clinical care, similar processes are repeated with some given more emphasis than others. For the purposes of documentation, each phase can be thought of as being divided into segments corresponding to the the processes involved in clinical patient care as tabulated below:
| No. | PHASE | SEGMENTS |
|---|---|---|
| 1 | Phase of determining the diagnosis and immediate care | – initial data gathering – determination of diagnosis – immediate or early treatment – start monitoring |
| 2 | Phase of initiation of definitive care | – select and modify care plan – initiate definitive care plan – continue monitoring |
| 3 | Phase of optimization of care | – review progress and response – review compliance – review complications – modify plan, improve care |
| 4 | Phase of maintenance of care | – continue care as planned – continue monitoring – review progress |
| 5 | Phase of resolution | – measure outcome – determine if problem resolved – continue care if unresolved – discontinue care if resolved |
How the clinical care processes are segmented into phases is depicted below:

The decision to proceed from one phase to the next depends on whether the objectives of the former have been achieved. In an emergency case, the initial phases are compressed such that tasks within them such as resuscitation and stabilization are accomplished within a short period. In non-urgent cases the phases are stretched over a longer period.
Even though tasks are performed to achieve the objectives of a phase, it does not mean they are confined to thatphase. Many tasks must be continued to maintain the gain achieved. For example, the initial data gathering is followed intermittently by progress assessment. Symptom relief may be necessary even at later phases or even permanently. Monitoring is done continuously until the parameters are stable and is unlikely to change. Stabilization and optimization must continue and the patients condition must not be allowed to slide.
How the care episode is divided into phases is depicted below:

In the in-patient setting some of the procedures may be performed continuously where necessary or intermittently. In the outpatient setting, most procedures will be performed intermittently with continuity being facilitated by self-care, home care and may be teleconsultation.
Cases can be categorized into acute or chronic categories. Each categories can be divide further into sub-types based on severity, grading, stage at presentation, and response to treatment. The differences of their care is mainly in the mode of treatment and intensity of monitoring. As such, the care of the disease sub-types are designed as as separate alternative blocks or modules.
When the SOP/Care Plan is documented, the narrative differentiation into alternatives take the form of separate segments designated by sections and paragraphs with appropriate headings as shown below:
In the Reference SOP/Care Plan each phase can be thought of as groups of tasks to be performed to achieve a particular objective.
- Care episode
- Phases
Selection of / Content of Each Phase of the SOP/Care Plan
Since moving on from one phase to the next depends on whether all tasks has been performed and the objectives have been met, the content of each phase need to be determined with this consideration in mind. There may be occasions when tasks of one phase is carried over to the next. Some tasks like monitoring persists through out the phases. Adoption of the division into phases is critical in determining the structure, content and implementation of the SOP/Care plan.
- Care episode
- Phases
- Clinical Care Procedures
- Phases
PHASE 1: Phase of Determining the Diagnosis and Early Treatment
This is the phase of initial contact with a health care provider. The procedures are grouped to serve two functions with both running concurrently.
- formulation of diagnosis
- immediate or early treatment (resuscitation, support, symptom relief)
The phase start with the procedures of establishing the reason for visit. A triage procedure is included in the plan when necessary. Guidance to the front-end staff at reception or triage regarding the criteria to differentiate disease conditions requiring urgent (emergency) care as opposed to diseases that can be cared for at a more comfortable pace (non-urgent or elective cases). Based on it care providers should be able to:
- determine whether to direct the patient to immediate care or give an appointment the appropriate
- determine the appropriate clinical unit to accept the case
- choose the appropriate setting (emergency, outpatient, in-patient) for the care to be given.
Clinical data Gathering
The encounter with a clinical care provider can be with a nurse of a doctor depending on the type of case. The information to be gathered is aimed at making a preliminary diagnosis (symptom complex, clinical syndrome, diagnostic related group) and assessment of the condition of the patient.
The latter depends on whether the disease process is at an early or later stage of its natural history, depending on whether the patient seeks treatment early or late. Early treatment is given based on the working diagnosis (symptom complex, clinical syndrome, diagnostic related group) even as efforts at determining the definite diagnosis are being made.
Formulation of Diagnosis
The main objective of this phase is to determine the diagnosis as accurately and comprehensively as possible. For a new case where the diagnosis is not known, steps are taken to identify it. This process can be termed as the formulation of the diagnosis. Hence, the steps for this purpose are:
- clinical data gathering (interview and examination)
- performing simple tests
- initiation of observations and monitoring
- determining the working diagnosis
- Care episode
- Phases
- Clinical Care Processes
- Data gathering
- Determination of Diagnosis
- Planning
- Execution of plan (treatment, monitoring)
- Review of outcome, treatment, diagnosis and plan
- Continuation or discontinuation
- Clinical Care Processes
- Phases
At the beginning, a clinician takes charge of the case and is said to be the primary provider. Usually this person is the doctor to whom the case is assigned. However, depending on the scope of care, he/she can be a nurse, nurse practitioner, therapist, or clinical psychologist (or other practitioners). The primary provider is responsible for formulating the diagnosis. The working diagnosis at this stage is usually provisional and may take the form of a symptom complex, clinical syndrome or a disease related group. Plans must be devised for them so that they can be referred to with the change in diagnosis as the care progresses.
Process of Determining the Definitive Diagnosis
The provisional diagnosis will provide a guide to the next step which consists of:
- taking a more elaborate history
- finding out more about specific symptoms
- closer examination of regions or organs involved
- performing more specific and elaborate diagnostic investigations
- analysis and interpretation of all data available to formulate the definitive diagnosis
The clinician in charge uses the data from tests, observation and the monitoring to arrive at the definite diagnosis. The diagnosis need to be further refined to clarify the variant of disease, severity grade, stage of illness, risk stratification and prognosis.
Investigations are aimed also at determining the patient’s general physiological status and functions of various systems besides focusing on determining the system or site involved or the likely pathology and in the end, the definitive diagnosis. Providers of clinical support services become involved when diagnostic investigations are ordered.
The definite diagnosis is one that is both specific and certain. Often, the effort to determine it takes time. This phase may be completed over a few sessions with intervals between the sessions. This is necessary because tests have to be scheduled. The results of pertinent tests or observations are not immediately available but are obtained at different times and have to be accumulated. analyzed and interpreted before the conclusion is made regarding the diagnosis. Depending on results additional tests may have to be done.
However, every effort must be made to obtain a definitive diagnosis because it indicates the cause of the disease or at least the pathological processes that are affecting the patient. This information is necessary before the plan for specific treatment can be made. In fact this phase ends only when a reliable working diagnosis is arrived at.
Immediate Care and Early Treatment
Therapy must not wait for want of an accurate diagnosis. The plan for immediate care and early treatment is based on the working diagnosis which at this point of care is provisional in nature and are likely to be:
- a symptom complex
- a clinical syndrome
- a disease identified to belong to a diagnostic related group
SOP/Care plans are prepared for these levels of diagnoses. Only occasionally, the specific diagnosis is obvious from the start.
Procedures to be Performed
Generally in both acute and chronic illness, procedures at the immediate phase should include:
- nursing care
- immediate and continued relief of symptoms
- monitoring of relevant parameters
- maintaining normal physiology through resuscitation and stabilization
- providing nutrition or at least fluids and electrolytes,
- giving support (physiological, psychological, social and spiritual)
- taking preventive actions
- avoiding and reducing emergence of disability
- treatment of ongoing problem as they arise
The outline of the workflow for this phase is depicted below:

The difference in approach between acute and chronic illness is a matter of intensity and priority. In an acute illness resuscitation, stabilization of physiological parameters and support of their functions must be done quickly., In a chronic illness these can be done in a more measured manner.
PHASE 2: Phase For Initiation Of Definitive Care
This phase is a direct continuation of the previous phase. Only when the diagnosis is definite can the direction of care be set clearly. Plans are designed according to the needs posed by the specific disease, illness or health problem. As such, the guidance given can be more definite (certain and specific). It has to take a more didactic tone and be more regimented. From this point the care for the rest of episode is concerned with the initiation, optimization and maintenance of definitive care.
Design of Care Plan based on Definite Diagnosis
The plan for definitive care should allow allow the care provider to know the objectives of care (expected outcome, therapeutic end points). A more definite SOP/Care Plan appropriate to the diagnosis must be constructed for various diseases and their variants. The plan should include continuing efforts to refine the diagnosis and further clarify the variant of disease, severity, grade, stage of illness, risk and expected or desired outcome. Plans for the these variants need to be prepared.
Plans should cater for unexpected developments, eventualities and contingencies that may occur. Some of these can be anticipated such that the care provider must be guided on on decisions to make when they occur. However, it quite likely that the care provider need to address them at his/her own discretion.
In this phase, the care provider should be reminded to continue tasks like nursing care, symptom relief, monitoring, support and others initiated earlier. Regular observations and monitoring should be a regular activity.
Setting the Objectives of Care
Treatment end points need to be defined and measurements made to determine whether these end-points have been achieved. Depending on the disease, the objective of treatment would be the combination of any of the following:
- cure the illness,
- contain it or control the progress and minimize complications
- mitigate the effects
SOP/Care Plan is designed to be consistent with the care objectives consistent with the disease encountered. The care plan helps the care provider define the treatment end points, and choose the most suitable treatment approaches or modalities. In this phase and in later phases. the care plan should indicate the measurements to be made to determine whether the end-points have been achieved. Advice should be given on the parameters to be used to review the progress of the patient. It should include efforts to detect deterioration or improvement and occurrence of complications of illness or treatment. The frequency ( regularity) of measurements should also be indicated.
Depending on the illness, this phase may spread over a considerable period and at different service delivery settings. In the case of an acute illness, efforts should be made to complete this phase as early as possible. But for elective cases, it may be possible or necessary to have the patient discharged at the end of the visit (e.g. in-patient care) and to complete it in the next visit (e.g. at an outpatient setting). For less acute cases this phase may be carried out entirely at outpatient settings and over a few visits.
Procedures to be Performed
In this phase almost all care providers are involved directly or indirectly in the care. Therefore procedures would be allocated accordingly and listed in their Task lists. These tasks include:
- review of data
- ascertain diagnosis
- choose and execute appropriate plan
- start definitive treatment
- monitor and observe
- initiate preventive measures
- initiate rehabilitation
- provide education and counseling
The tasks involved and their sequence is as shown below:
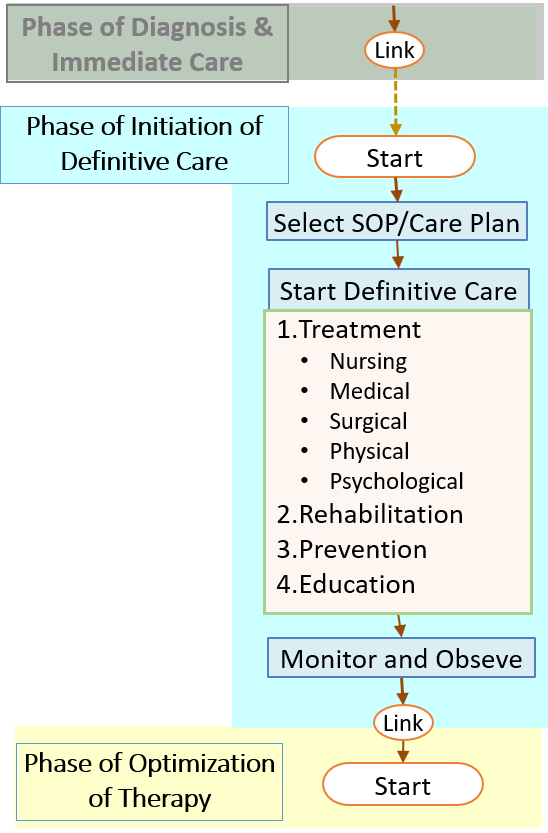
PHASE 3: Phase of Optimization of Care
The main aim of this phase is to optimize the benefit of care given. The care provider need to be made aware of the desired treatment end points and provided with the means to achieve them.
Progress is assessed through:
- review of symptoms and signs,
- observations,
- monitoring,
- repeated investigations
Assessment are designed to address both the progress of the disease and effect of treatment. The way results are presented for the various parameters is proposed. The plan should help the care provider to analyze and interpret the results and determine the behavior of the disease and improvement or otherwise of the health of the patient. The care provider must be given the criteria to be used to determine whether care has been optimized. In general, optimization is considered achieved when the care regimen produces the best possible level of benefit. If optimization is not achieved the care provider is advised on how to make adjustments and modifications to the care plan.
Conformance of the care providers to the plan must be assured through quality control measures. Compliance of patients to instructions must also be assessed and enforced.
The phase may extend beyond one session. If the the patient is at first managed as an inpatient he/she may be discharged and the care continues in the outpatient setting. The progress of acute illness is often dramatic and easily discernible. The progress of chronic diseases vary in many ways including:
- slower speed of deterioration or improvement ,
- active vs inactive periods (remission, reactivation),
- emergence of complications of the disease
Measurement of outcome and comparison with planned targets is an integral activity of care at this stage. Scoring systems and check lists can be mandated or suggested. If the progress is satisfactory, the plan is continued with further improvement if necessary. However, if it appears to be ineffective, guides on how to make minor or major modifications must be provided. If there is doubt regarding the diagnosis further investigations must be done, If the diagnosis is different, a new care plan need to be initiated and optimized.
Optimization is considered achieved when the care regimen produces the best possible level of benefit. The plan is then continued.
Procedures to be Performed
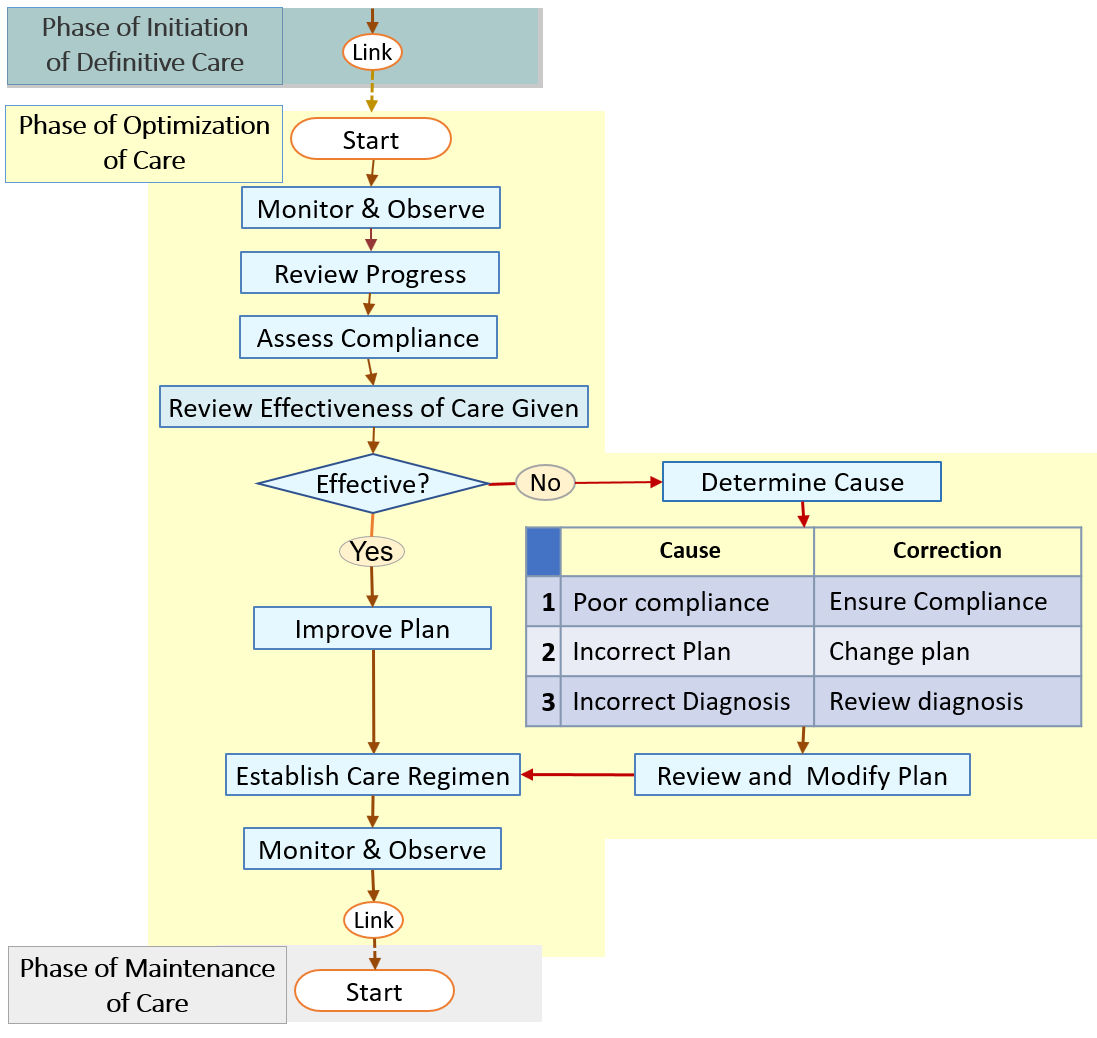
PHASE 4: Phase of Maintenance of Care
Moving from initiation and stabilization of definitive care to the maintenance phase depends very much on the effectiveness of the care given or improvement in the disease condition. Otherwise, the care persists in that phase. It must be noted that a phase may need more than one visit to complete.
The care provider must maintain the plan of care that led to the optimal level of outcome. Depending on the illness, this phase may extend over a considerable period. Usually, it is conveniently carried out at outpatient settings (clinics, day, care, home care, teleconsultation. self care).
The care provider is expected to follow the established care regimen as closely as is possible. At the same time, an important aspect of the plan is the continued evaluation of response to and effects of therapy. The following factors are assessed:
- conformance to the plan by care providers
- patient compliance
- detrimental effects of therapy
The progress of the patient is reviewed regularly to detect deterioration or improvement and the occurrence of complications of illness or treatment. An important aspect of this phase is determining the appropriate intervals between reviews.
The effectiveness of the care given may not be maintained for reasons of:
- poor compliance,
- change in the disease,
- change in the patient’s general health
The care provider may have to revise the SOP/Care Plan and modify the treatment accordingly. Also, he/she should consider reviewing the diagnosis especially in terms of the severity and grading which would then require modification of the objectives and the plan. It is also possible that failure to achieve favorable outcome, even at this stage, may be due to a wrong diagnosis.
For illnesses that has been brought under control, the plan should provide care provider with the indicators to look out to determine deterioration or recurrence.
Procedures to be Performed
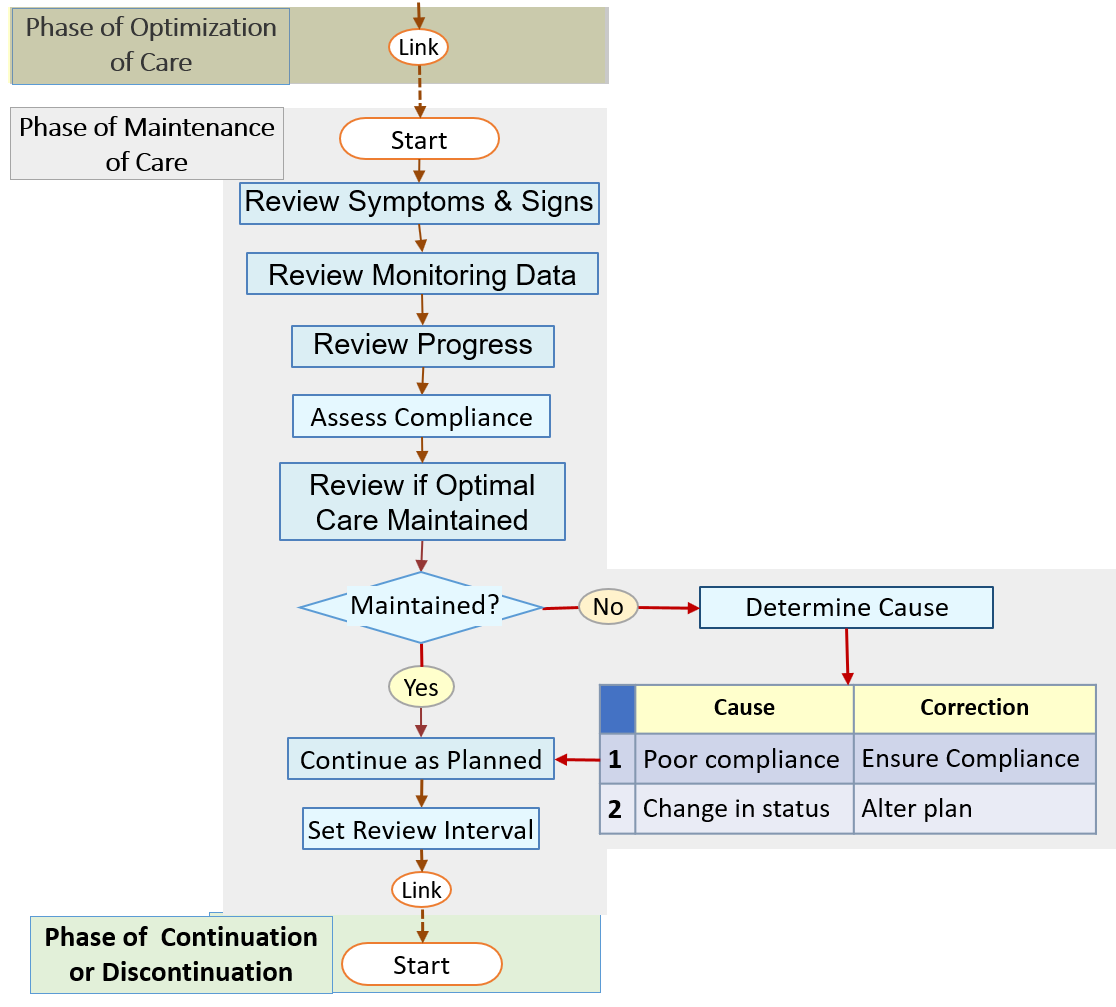
PHASE 5: Phase of Resolution (Continuation or Discontinuation of Care)
The plan should indicate to the care provider at what point decision should be made on whether the patient requires further care. The criteria used are based on the resolution of the illness or the achievement of the optimal outcome. In practice, this means the decision to continue follow up visits. There is no advantage in putting the patient on regular follow up when it is unnecessary. However, access to the service can still be offered on a needs (prn) basis.
Depending on the nature of the illness and the response to care, the service may reach a stage where it can be discontinued. This is so with curable diseases.
On the other hand, chronic illnesses are characterized usually by continuous progression or persistence. The duration of care is therefore long term and usually extend throughout the life of the individual. Some diseases may resolve, go into remission and be dormant only to appear again later. Temporary cessation of therapy with planned follow up reviews at longer intervals (quarterly, half yearly, or yearly) may be necessary.Some diseases may not require care at health care facilities but sufficiently managed by self care. Rarely some chronic diseases runs through its course and dissipates. The care can then be phased out.
For illnesses that has been brought under control the care provider must be on the look out for recurrence.
Procedures to be Performed
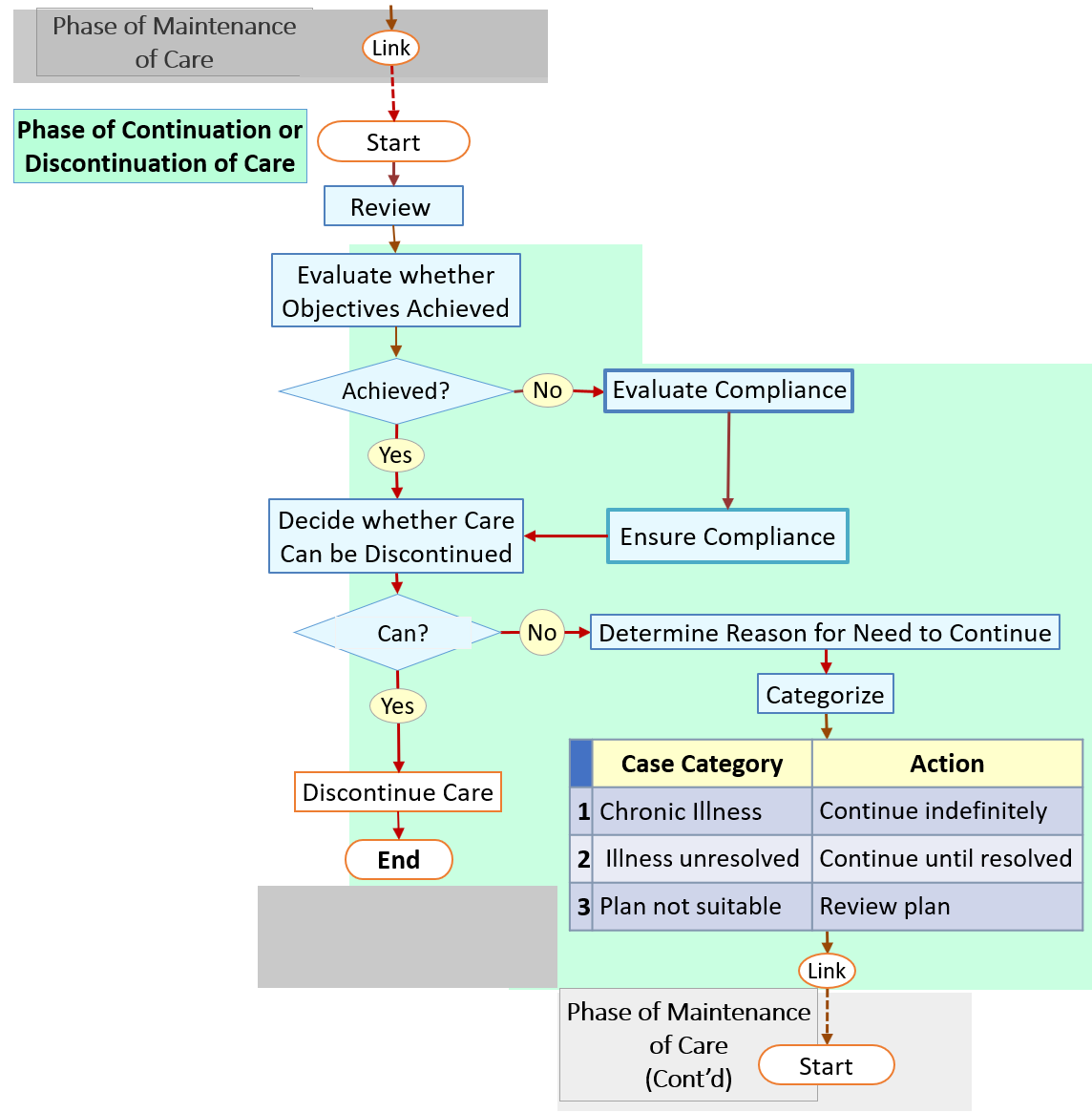
The circumstances that allow care to advance to the next phase often become evident when actual care is given and the care provider has reviewed whether all efforts planned has been performed and after the outcome of tasks are known. Hence it will be discussed in the discussion on the Actual OP/Care Plan.
Documenting Phases as Segments of the Reference SOP/Care Plan
The Reference plan document should be divided into segments consistent with phases with each segment indicating the sets of clinical care processes to be performed. The care provider must be aware of the phase of care that he/she is currently in. If the Reference SOP/Care Plan is written on paper, each segment need to be marked out clearly as paragraphs with clear headings. In a computerized system, it is possible for the relevant segment to be called for (via a menu) or be automatically presented to the care provider at the appropriate time.
How the structure and content of the SOP/Care Plan is segmented in accordance with phases is shown below:
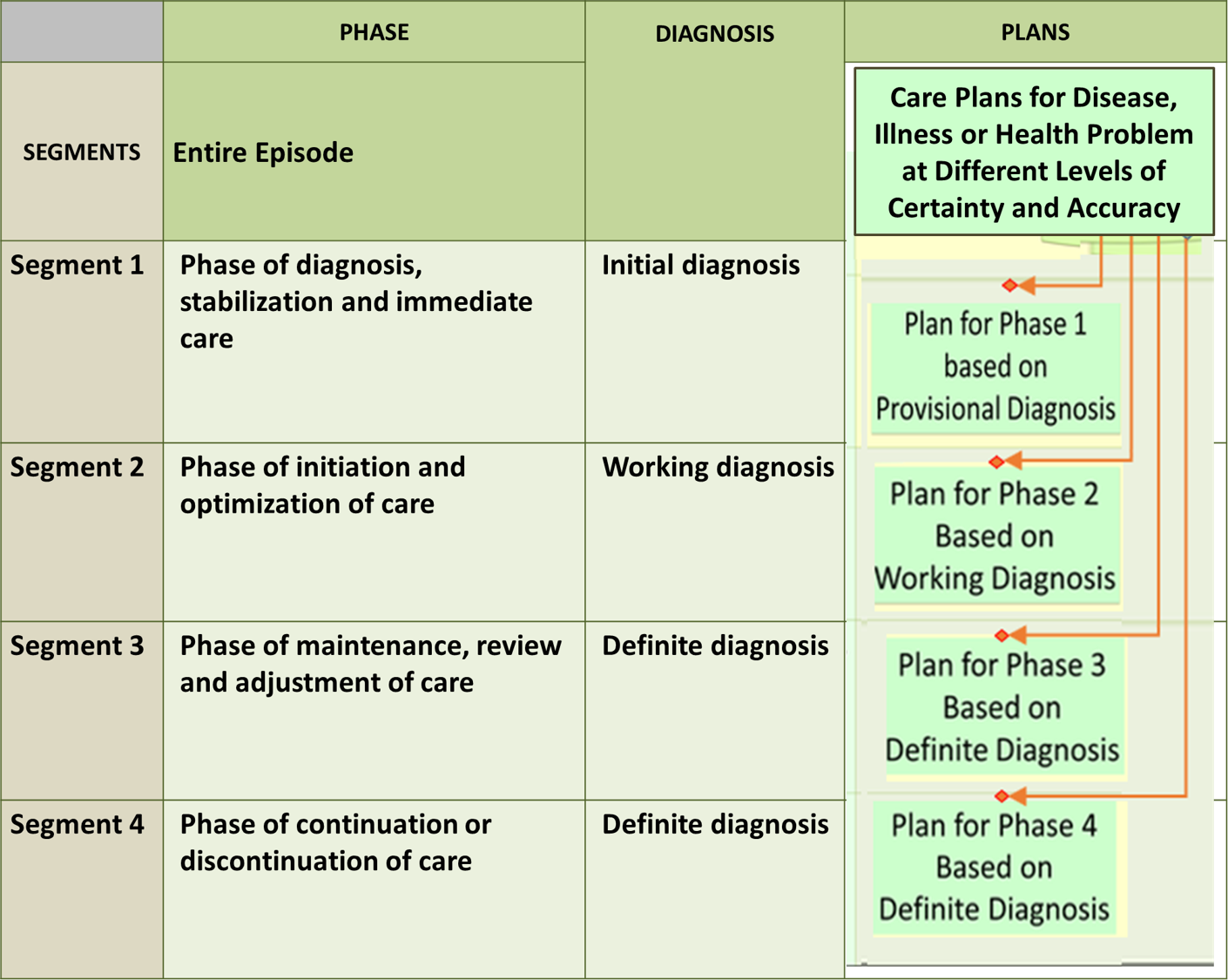
It must be noted that, because plans change with the change in diagnosis, the Actual plan is a composite plan built incrementally by adding on segments derived from plans for the symptom complex, clinical syndrome, disease group and specific disease. The plan is therefore dynamic. As new plans are adopted, new items will be added, some items in the previous plan are retained while some others are discarded. The plan is only completed at the phase of definitive care when the definite diagnosis is ascertained.
The decision to progress from one phase to the next is a decision-making process requiring much thought, In a computerized system, the criteria to indicate the right moment to move on is the fulfillment of the objectives based on data regarding progress and outcome. Even then, the decision remains the responsibility of the care provider. Completion of a phase may require a variable number of sessions and hence cannot be scheduled in advance.
