
Outline of Structure and Content of SOP
Standard Operating Procedures are documented as descriptions of how work is to be carried out for a specific category of patients defined mainly by the diagnosis. Each is used as a source of reference. necessary components and the way they are laid out is as outlined below:
General Principles
Standard Operating Procedures (SOP) / Care Plans when documented has the following purpose and characteristics:
- The set of SOPs are applicable to a specific organization
- One SOP is used for one service product
- SOP / Care Plans is written for syndromes, Specific diseases as well as their variants
- While advocating uniformity and standardization it allows for variance
The general structure and content of the SOP / Care Plans is as outlined below:
| No: | Section, Paragraph | Content |
|---|---|---|
| 1. | Title | Name of the service product for which the SOP / Care Plan is applicable |
| 2. | Service Product | Description of the Service product A. The typical patient group for whom the SOP/Care Plan is applicable B. The Needs of the patient to be served ___a. Primary Diagnosis ___b. Disease Complexity (type, grade) ___c. Severity Level ___d. Stage of the Disease. C. The location where and the care providers who provides the service |
| 3. | Objectives and Standards | A. General objectives. B. The desired Outcome ___a. the intermediate outcome standards ___b. the final outcome standard |
| 4. | Service Delivery System | Indicate the requisites for successful conduct of care a. Facility, Environment b. Necessary equipment c. Staffing |
| 5. | Policies and Procedures | A. General policies statement B. Description of procedures and operational policies in narrative format. and Depiction of Workflow in graphical format. ___a. Segmentation into Phases of Care ___b. Division into sessions …….. (Episode, Visits, Events) ___c. Means of execution ……..(Work Schedule Orders, Task lists) C. Supplementary instructions ___a. Guide to decision making. ___b. Guide to documentation ___c. Reference documents _____ i. Work instructions _____ii. Specifications and Standards _____iii. Forms and Charts |
| 6. | Quality Control | Quality Control Methods a. Methods to Ensure Conformance b. Preventive measures c. Quality Measurement d. Comparison with Standards ….(Detection of non-Conformance) d. Rectification and damage control |

The structure and content of each part are described below.
Title
The title is the name of the Service Product for which the SOP/Care Plan is to be applied
From the title, the reader should be able to select and match the appropriate plan to use for a patient be it for a specific disease or for a symptom complex or syndrome. health problem and for a particular phase. The title is a very concise statement indicating the patient type, the diagnosis or indication. To clinicians, the ‘care’ or ‘the management of a patient’ is the provision of the entire service or care for a particular patient according to his/her needs which are determined largely on the identified diagnosis or health problem.
The model plan is generic in application. Conversion of such plans is done when the actual care of an individual patient is provided.
Description of the Service Product
Following the title, what the service is for (the indication) and what is contains is described briefly.
As such, the Service product consists of a well-defined set of services to be provided for a typical patient (case) who has an episode of a specific illness. This is, to a certain extent, still generic and would need customization, by additions or omissions, when it is used as the Actual SOP/Care Plan in the actual care of an individual patient.
and the context such as the phase of care, the service delivery setting where the service is to be given (inpatient, outpatient and day care) and the type visit or encounter.
- The patient group for whom the SOP/Care Plan is applicable. It can be:
- A typical disease, illness or health problem.
- Variants of the disease (as defined by Severity Level, Stage of the Disease, Aetiology, etc.)
- The Needs of the Patient to be served
- Primary needs (Effects and complications of the disease)
- Secondary needs
DIAGNOSTIC CRITERIA
The service product and therefore the choice of the appropriate SOP/Care Plan is based on the diagnosis. As such it is imperative that a correct diagnosis is made. A diagnosis is arrived at by interpreting certain variables including signs, symptoms, the results of clinical tests, investigation findings (laboratory, imaging, and endoscopy), monitoring parameters, clinical progress and response to treatment. Through research and experience, the medical profession has identified sets of variables that predict a diagnosis i.e. the ‘diagnostic criteria’. This knowledge can be presented (as decision support) to care providers to aid them in making a diagnosis. In certain instances, especially when a scoring system is used, these predictions have a high level of accuracy. However, a rough guide can be also of use to the clinician.
Objectives
The care given as described in the SOP/Care Plan is aimed at achieving two main groups of objectives, each having their own defining characteristics:
- desired outcome from the patient’s view point which includes:
- effectiveness
- appropriateness
- safety
- acceptability (accessibility, affordability)
- the output of the service from the view of the healthcare facility i.e.,
- productivity
- efficiency
- viability (cost-effectiveness, sustainability)
A statement specifying the objectives of clinical care is essential for every SOP. These may include:
- expected outcome or treatment end points (targets, limits and quality standards)
- the intended degree of restoration or amelioration of the disrupted quality of life (ability to: work, enjoy leisure, attend school and do daily life activities)
- avoidance of side effects or complications of treatment
Policies and Procedures
Description of Policies and Procedures is the main part of the SOP/Care Plan.
- A textual description (narrative)
- A work-flow chart
When designing the SOP/Care Plan, starting with the narrative description is the best way to go. However, when presenting it as the final document it may be better to show the graphical workflow first.
General Policies
General policies provide the limits or constraints within which the facility delivers its service taking into consideration the values held by it. The general policies are stated in a separate paragraph. They should indicate:
- philosophy, aspirations, goals and principles of the facility/organization
- requirements it follows in terms of
- laws and regulations
- professional standards
- ethical considerations
- Methods, modalities and technology it utilizes
- the service delivery system it provides (expertise, material, machines, equipment)
Procedures and Workflow
The whole work procedure needs to be described in text format. In general, the description takes the form of a sequential list of instructions on how to perform tasks or individual processes and the policies that guide it. At the same time the direction, input, technology to be used, persons assigned to perform the task and the expected outcome of the procedure (the intermediate outcome) are specified.
The sequence, direction and layout of processes or tasks that makes up a procedure must be described clearly and in detail. It is best written before or at the same time as the flow chart is being drawn. In a general sense, the textual description explains each workflow symbol (boxes, arrows etc.) but more importantly, it states the specifications and standards of the care process as well as the operational policies that govern them. Therefore, it is the principal component of the SOP/Care Plan.
Operational Policies
At the operations level (i.e. when work is performed), the general policies of the institution or service unit are translated into operational policies which define goals or objectives as well as the limits within which tasks or processes are performed. These limits (rules, regulations, targets and standards) may relate to efficiency, quality, costs, responsibilities, preferences and exceptions.
The operational policies guide and constraint the procedures and processes. They include indications or contra-indications, alternatives, allowable variations and contingency plans, rules and criteria for choosing one path or another. Statements regarding these policies are embedded within (i.e. written together with) the instructions on how to carry out procedures. The operational policies are written together with the instructions on how to carry out procedures.
WORKFLOW
In the SOP/Care Plan, the path/flow/sequence/layout of clinical processes is presented in two ways i.e.:
- a description of how procedures are sequenced or laid out, written as a narrative,
- depicted graphically as a chart
Narrative (Textual Description) of Procedure and Workflow
The procedures and the workflow is first expressed in narrative form. It describes the arrangement of the tasks for the delivery of a service in terms of content, layout, sequence and direction. The operational policies are embedded within it.
The general flow of the main tasks are as listed listed below. They need to be elaborated according to the peculiar requirements of the delivery of the service service product: need to be .
- Acquisition and documentation of clinical data (Initial Assessment, Progress Notes)
- Acquisition and documentation of data obtained from various investigations
- Analysis and interpretation of available clinical data
- Deriving conclusions regarding the patient’s health problems (the diagnosis) and documenting it (including severity grading, staging)
- Monitoring and charting of clinical parameters (Observations, serial measurements )
- Planning the management and documenting it (with decision support)
- Implementation of plans: Placing orders and carrying out tasks (Performing Investigations, treatment, administering drugs)
- Documentation of results, procedures performed, findings, and outcome
- Review of (monitoring and test) results and interpretation
- Quality Control Procedures (e.g. check lists)
- Progress review, assessment of outcomes
- Communications (Referral Notes, Replies), requests and orders
- Writing Summaries
Describing Sequential Vs Simultaneous Tasks
Tasks need to be sequential if:
- the tasks require the patient to cooperate by physical or verbal means,
- care providers have to take turns to perform them.
This is because a patient can only be at one place or interact with one care provider at one time.
Tasks that do not require the presence of the patient can be done simultaneously or concurrently. Examplesinclude
- tests on samples taken from the patient,
- cognitive tasks such as analysis and interpretation of data (for diagnosis, decision making)
- administrative tasks such as making virtual changes in computer applications, prior to the actual action, such as adding a patient to a schedule, moving the patient, and making an administrative discharge,
How and when tasks are performed simultaneously need to be addressed in SOP/Care Plans.
General Sequence of Procedures
This general workflow is applicable to most cases. However the sequence of the processes does not necessarily follow this strictly but will depend very much on the type, severity, urgency, speed of progress and effects of the illness. In an urgent case, emergency treatment is given first before a full interview, examination and tests are done. Some cases may have obvious diagnosis based on routine tests or chance findings from investigations already done during other instances of care. As such, it would not be necessary to repeat the diagnostic investigations. For some types of cases, it may be more practical to perform certain processes first as a routine for example performing urine tests at a antenatal visit or visual acuity measurements for every case with a problem of vision.
Guide to Decision Making
The workflow has decision making steps i.e. points when care providers have to choose the appropriate path when alternative directions exist. The decision is guided by criteria such as:
- policies,
- judgement,
- patient preference,
- availability of resources.
Supplementary Documents
- Workflow, and links to related SOP/Care Plans
- Phases of Care (Episode, Visits, Encounters, Tasks and Events)
- Work Schedule (Orders, Tasks, Task , Time table)
- Guide to decision making
- Guide to documentation
DOCUMENTING PHASES AS SEGMENTS OF THE REFERENCE SOP/CARE PLAN
The Reference plan document should be divided into blocks consistent with phases. Each block is indicated by a section heading. The block in turn consists of segments with each segment indicating the sets of clinical care processes to be performed. Segments may have paragraph headings. The care provider must be aware of the phase of care that he/she is currently in. If the Reference SOP/Care Plan is written on paper, each segment need to be marked out clearly as sections and paragraphs with clear headings. In a computerized system, it is possible for the relevant segment to be called for (via a menu) or be automatically presented to the care provider at the appropriate time.
The Work flow Chart
Besides describing the path/flow of how the service is given as a narrative, it is also depicted graphically. It may be better to present the workflow before the text description but the idea is for the user to switch from one view to the other regularly. An example is shown below:
- Workflow, and links to related SOP/Care Plans
- Phases of Care (Episode, Visits, Encounters, Tasks and Events)
- Work Schedule (Orders, Tasks, Task , Time table)
- Guide to decision making
- Guide to documentation
General Outline of the Workflow (High Level Workflow Chart)
A general outline of the workflow is often called the high level workflow or ‘critical’ pathway. When the processes are complex it is beneficial for better understanding to demonstrate the flow initially in the form of an outline depicting groups of tasks.
details are elaborated subsequently.
The Full Workflow Chart
In the SOP/Care Plan, the understanding of the flow, sequence and layout of clinical processes is much enhanced if depicted graphically as a workflow chart. However, it must always be preceded or followed by a narrative description. The workflow that can be applied generically for patient care is as depicted below:
Depicting Simultaneous Tasks
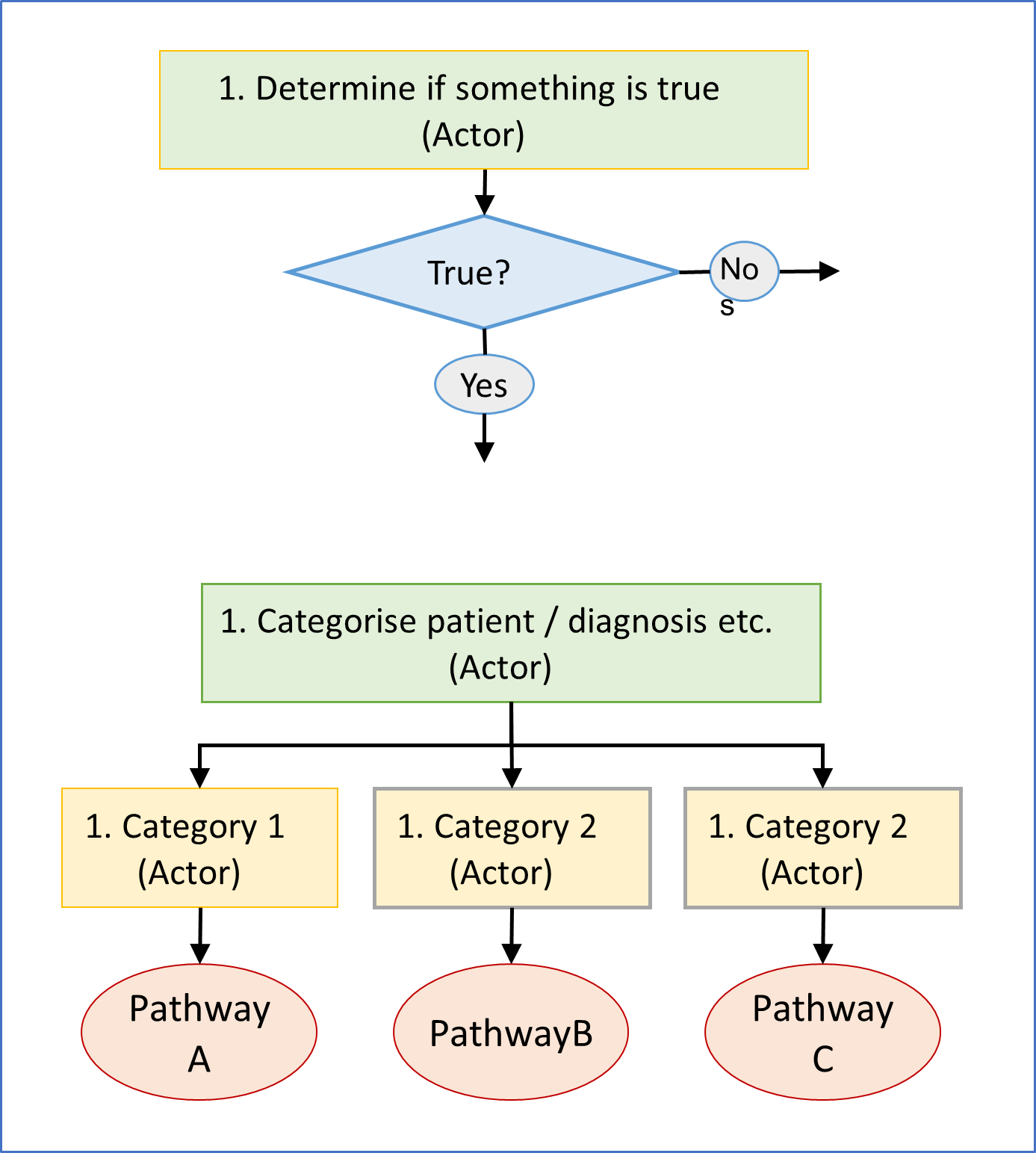
Depicting How Decisions are made and Alternative Actions
Indicating points where a decision must be made on choosing alternative paths. Pointers to decision making
11.2 Decision Making Steps an Essential Component of the Workflow
Decision making steps is an essential component of the workflow because its determine the direction of the steps of the care process.
In clinical care, the plan is very much dependent on diagnosis. After selecting a plan based on the initial diagnosis, the care provider may decide to alter or revise the plan based on the criteria listed below:
- Changes in the understanding of the illness affecting the patient (the certainty and comprehensiveness of the diagnosis )
- Evolution of the disease along its natural history,
- Advancement of the flow of clinical processes,
- Occurrence of other emerging issues (incidents, contingencies)
There are instances when the workflow cannot progress according to the initial plan due to various impediments or circumstances. At times, the processes e.g. information gathering, investigations or tasks have to be repeated or abandoned. In those cases or if the prescribed treatment plan is ineffective, unacceptable or unsafe for the patient, an alternative approach or modality is used. Non-compliance by care providers or patients is also a factor that affects the progress of the workflow as well as the success in achieving the desired outcome.
11.2.1 Decision-Making and the Resultant Change in Plan
Decisions are made when there are choices or options to be selected. In clinical care, decisions are made based on conclusions arrived after appraising the situation based on accumulated information. The conclusion may be determined by appraisal of:
- the updated working diagnosis
- the latest understanding of the disease/problem,
- the evolving objectives of care,
- the progress of the disease,
- the response to treatment.
The choices or options that a care provider can make are: - to retain the current plan without alteration,
- to make modifications to the current plan,
- to change the plan completely to a new plan.
Blocks CORRESPONDING TO PHASES OF CARE
Cases can be categorized into acute or chronic categories. Each categories can be divide further into sub-types based on severity, grading, stage at presentation, and response to treatment. The differences of their care is mainly in the mode of treatment and intensity of monitoring. As such this variation in care of the disease sub-types is written in the document as alternative segments designated by sections and paragraphs (with headings) as shown below:
Blocks and Segments
The Reference plan document should be divided into blocks consistent with phases. Each block is divided further into segments made up of sets of clinical care processes to be performed. The care provider must be aware of the phase of care that he/she is currently in. If the Reference DOP/Care Plan is written on paper, each block marked out clearly as sections with clear headings and each segment as paragraphs. Hence a section will have many paragraphs. In a computerized system, it is possible for the relevant segment to be called for (via a menu) or be automatically presented to the care provider at the appropriate time.
Depicting the Work Schedule
Work is the expenditure of energy to produce a useful outcome. It is made up of a series of tasks performed by workers which in patient care are called care providers. The work can be done manually or with the help of machines. There are instances when the work is done by machines initiated by instructions given by a worker or automatically based on instructions built into applications. These instructions are called orders.
The activities (processes, tasks) within the SOP/Care Plan is broken down into sets relevant for particular scheduled periods (visits or encounters) or phases of care. This is the schedule of implementation of the SOP/Care Plan and it contains:
- a heading indicating the purpose for which it is used i.e. the health problem, the phase of care and any other indication
- objectives and expected outcome
- a list of all tasks grouped according to the method or technique or the professional competency
Task Lists
From the SOP/Care Plan the tasks assigned to a particular care provider (the same person or another person from the same professional team) can be listed. This list called the Task List guides the care provider on his/her contribution to the care of the patient and when it is to be performed.
In a paper based system, the list is created manually (e.g. on a piece of paper or written into the medical record) at the time of initial assessment or progress review. The list acts as a reminder. The care provider must at all times be aware of the progress of the work process and also of any changes made to the plan by the team leader or any other care provider..
In a computerized environment, what is to be done according to plan is listed as a set orders called the Order Set. These list of orders are generated automatically but can still be amended to vary the urgency, frequency, duration, location and assignment. Depending on who is responsible for performing the task, Task lists are ten generated for each named care provider or for a care team belonging to a professional category.
Thus, Task lists are the means for executing the SOP/Care Plan. Care providers must be aware of the tasks that have been completed and those that are still pending. When a computerized system is used, the system is able to indicate the status of performance and provide reminders through prompts and alerts.
Task List for One Patient
From the SOP/Care Plan the tasks assigned to a particular care provider (the same person or another person from the same professional team) can be listed. This list called the Task List guides the care provider on his/her contribution to the care of the patient and when it is to be performed.
In a paper based system, the list is created manually (e.g. on a piece of paper or written into the medical record) at the time of initial assessment or progress review. The list acts as a reminder. The care provider must at all times be aware of the progress of the work process and also of any changes made to the plan by the team leader or any other care provider..
In a computerized environment, what is to be done according to plan is listed as a set orders called the Order Set. These list of orders are generated automatically but can still be amended to vary the urgency, frequency, duration, location and assignment. Depending on who is responsible for performing the task, Task lists are ten generated for each named care provider or for a care team belonging to a professional category.
Thus, Task lists are the means for executing the SOP/Care Plan. Care providers must be aware of the tasks that have been completed and those that are still pending. When a computerized system is used, the system is able to indicate the status of performance and provide reminders through prompts and alerts.
Organization of work Operations Management Multi Patient Task List View
Care providers usually provide care for more than one patient. The care set for a particular patient will consist of all or some of patient care processes. It may also include clinical administration tasks. For inpatients, these can be admission, referrals, transfer and discharge. For outpatients, these can be visit registration, follow up appointment, referral and discontinuation of visits.
ORDER SETS (CARE PACKAGE, CARE-SET, CARE-BUNDLE)
Reference documents
- Work instructions
- Specifications and Standards
- Forms and Charts
The SOP should contain reference documents that care providers can refer to when performing their tasks. The information provided should be endorsed officially by the organization . Examples of these include
work instructions or protocols
table of normal values,
percentile charts,
dosage regimens, food menu,
expected / control limits, standards, specifications,
regimens, recommended drug dosages and charges.
lists of drugs (official drug formulary)
glossary of terms ,
diagnoses terminology,
charge codes.
Care Plan 7
Care Process with Decision Support through Reference Documents
Work Instructions Or Protocols
Work Instructions or Protocols provide further details on how certain processes are to be carried out. They are predetermined didactic reusable instructions for performing a certain specific task or process as prescribed or endorsed by the organization. They are usually instructions describing how to:
Reference tables or lists may become part of this work instruction.
Since processes depicted by a work instruction would be performed in a similar manner at any time, location or for any indication, they may be compiled separately as an addendum to the SOP or kept in separate manuals/folders and only referred to if required. In a computerized system they can be reached through hyperlinks.
perform of-repeated routine tasks (insert a CV line, catheterize a patient, take a blood specimen, take consent etc.)
document (use of standard forms or charts, ),
operate machines (user manual),
use instruments,
use chemicals (safely and effectively),
order items (food, drugs, blood etc.)
serve or administer drugs,
transfuse blood or other infusions
other specific tasks
CATEGORIZATION, RISK STRATIFICATION / SEVERITY GRADING/ STAGING
Having made the diagnosis the clinician needs to clarify further:
which variant of the illness is affecting the patient
which stage of the natural history of the illness has been reached
what complications has accompanied the disease
how the patient has responded to the disease
As such, grading and scoring systems for various diseases should be adopted for each disease and the care plan should have variations for different severity levels, stages and grades.
5.1 GUIDE ON DOCUMENTATION of Clinical Findings and Results of Observation and Monitoring(USE OF FORMS OR CHARTS)
Relationship between Plan, Performance and Documentation
Pertinent data that is generated as results of tasks or processes must be recorded in standardized forms. In the SOP, guides are given on the use of various data documentation forms or charts used by the organization. Documentation forms should anticipate the data generated by the tasks within the SOP/Care Plan. In addition, the forms/charts also provide prompts/reminders for the care provider to perform certain tasks to obtain the data. Thus, the form itself acts as a decision support instrument
GUIDE ON DOCUMENTATION of Results of Tests
5.2 PROVISION OF CLINICAL DECISION SUPPORT
Clinical care is a knowledge driven and information dependent activity. Modern clinical practice must be re-engineered to take advantage of the advancement in knowledge and practice of clinical sciences, management science, and information and communications technology. Clinical Decision Support is the provision of guidance and knowledge at the point of care. It is an integral part of the SOP/Care Pln.
Clinical decision support is envisaged not as something separate but as built-in functions within the whole patient care. It is applied through several mechanisms:
Guide to the data that must be gathered and captured
Guide to making a diagnosis (diagnostic criteria)
Provision and matching of care plans for various categories of patients
Manual / Computerized analysis and interpretation of results (normal, abnormal, scoring, stratification, grading, staging, comparison with standards for quality control)
Provision of guides, instructions, alerts, prompts, reminders and suggestions,
before or during the performance of certain procedures
In response to certain situations, occurrences, incidents, non-conformance and abnormalities
indications and contraindications in use of a modality
Quality Control Quality Control Methods
- Methods to Ensure Conformance
- Preventive measures
- Quality Measurement
- Comparison with Standards
- Detection of non-Conformance
- Remedial measures
14 Style of the SOP/Care Plan
Special Considerations must be made in fashioning the structure and content of the SOP/Care Plan for different types of diseases and patients. Cases can be categorized further according to possible factors that clarifies a diagnosis such as Aetiological Type, risks, severity of illness, Stage at Presentation and Severity Levels and therefore prognosis. Categorization in turn allows the clinician to choose the right pathway and start an appropriate care plan. As such, grading and scoring systems for various diseases should be adopted for each disease and the care plan should have variations for different severity levels, stages and grades.
The pathological process disease varies with its aetiology. The causes of disease can be classified as:
- • Congenital
- • Trauma
- • Infection
- • Degenerative
- • Metabolic
- • Neoplastic
- • Change in physiology
- • Psychological
Each of these classes has distinctive presentation and needs. Therefore, different approaches are taken in the care of patients affected by them. For example, in cases of trauma particular attention must be given to supportive care and early treatment at the initial phase of care. In the later phases rehabilitation must feature prominently in the care plan.In an infection. identification of the causative organism will lead to a different therapeutic approach in the definitive treatment. Similarly in malignant neoplasm, the stage at presentation and the cellular grade influences the choice of treatment modality. Pregnancy, though not a disease, give rise to different physiological and sociocultural effects over its course. The phases of care are best divided according to trimesters.
Hence, the documentation of SOP/Care Plans for disease belonging to different classes with have different styles while that for diseases of a similar class can be planned in a similar manner.
14.1 Consideration for Stage at Presentation and Severity Levels
Patients seek treatment at different stages in the natural history of the disease. This is the main factor contributing to the severity level of the disease
(mild, moderate, severe or extent of involvement)
14.2 Consideration for Biological Profile
For many diseases, the presentation and the management is different for the paediatric vs the adult age group. Separate SOP/Care Plan must be designed for them. The same may be true if there is major variation in the disease and its treatment due to gender (e.g. Urinary Incontinence). Variation in the care when it happens in the elderly would probably require an addendum rather than a separate plan.
14.3 Consideration for Health Profile
risk factors, confounding factors Co-morbid Factors
If complete care is to be given, consideration should be given not only to the present illness but also health status before the illness began (pre-morbid status). It would not be necessary to design separate Reference plans to cater for these factors and circumstances. Instead, normally, they need to be considered when the Actual plan is formulated. The exception is when they are inextricably linked i.e. one do not exist without the other).
14.4 Disease Sub-Types and Corresponding Subset of SOP/Care Plans
The SOP/Care Plan can be written for the main disease if it has very minor variations in its presentation. Otherwise, as a rule, they would be written for a disease sub-type.
After designing SOP/Care Plans for a specific disease. variations must be developed for sub-types of it based on:
- the variants of the disease can be called the sub-types of it
- the different plans for the care of patients with these variants can be called the subsets of the SOP/Care Plan.
For example, Type 1 (Juvenile onset) Diabetes and Type 2 (Adult onset) Diabetes have dissimilar characteristics requiring two separate SOP/Care Plans. It is not appropriate to write one for Diabetes.
14.5 Building Reference Plans For Variants of the Disease
The disease can be identified as a variant at the start of the care process or later when more data are accumulated through:
- emergence of new symptoms and signs,
- physiological changes evident by change in parameters monitored
- investigation findings
- better exposure e.g. at endoscopy or surgery
- variation in the response to treatment
When the patient’s diagnosis is identified as a specific disease entity or a variant of it, the care that is provided for it would be the service product. For better understanding of the relationship between variants and the SOP/Care Plan associated with it, the following terms are used in this discussion:
Structure of SOP/Care Plans for Variants of the Disease
Creating alternative subsets of a SOP/Care Plan catering for variants or sub-types of the disease is a challenge. They can be designed and documented in two ways depending on the circumstances:
- as alternative segments to the main plan (applicable when the variation of the care of the various sub-types is slight)
- as a separate SOP/Care Plan, (applicable if there is a distinct difference in the care for the each sub-type of the disease)
Sub-types of the disease and corresponding sub-sets of SOP/Care Plans is depicted below.
Alternative SOP/Care Plans Corresponding to Variations in Patient Profile and Disease Pattern
14.5.2 Expressing Variations As Alternative Sub-sets of The SOP / Care Plan
When the variation in the case type and its care is distinct then separate SOP/Care Plans should be prpared. For example, Bronchial Asthma is categorized based on variation in acuity of onset into Acute exacerbation and Chronic (long term) presentations. The two categories are very different in the approach to treatment. As such, there is no value in having a SOP/Care Plan for Bronchial Asthma per se. However, separate SOP/Care Plans have to be designed and written for the two categories with the common parts shared. Separate SOP/Care Plans are also needed for care of Bronchial Asthma in children.
Each of the categories (acute or chronic) has further sub-types based on severity. The differences of their care is mainly in the mode of treatment and intensity of monitoring. As such this variation in care of the disease sub-types is written as alternative segments/paragraphs (with headings) as shown below:
SOP for Varieties of Bronchial Asthma
11.2.2 Changing To an Alternative Reference Care Plan In Response To Variations, Options and Contingencies
At the start of care (usually at the first session) the primary provider chooses a care plan that matches the diagnosis. At subsequent sessions the same plan may be used if appropriate. There may be a need to follow a sub-set of the plan depending on variations in the pathological grade of the disease, the stage of the disease, the level of severity or the emergence of complications.
Indeed, a Reference Care Plan for a different disease must be chosen in response to a marked change in the diagnosis.
Plans are also modified or revised if various other emerging needs appear. If formally designed plans are not available, then the care provider needs to devise the actual plans him/herself without referring to a Reference plan. Hence, it is better to design and put together a comprehensive library of Reference Care Plans to cater for various scenarios in the care of a patient for each disease, illness or health problem. The primary provider selects the appropriate plan from a library of SOP/Care Plans made available to him/her.
Structure of SOP/Care Plans for Variants of the Disease
Creating alternative subsets of a SOP/Care Plan catering for variants or sub-types of the disease is a challenge. They can be designed and documented in two ways depending on the circumstances:
- as alternative segments to the main plan (applicable when the variation of the care of the various sub-types is slight)
- as a separate SOP/Care Plan, (applicable if there is a distinct difference in the care for the each sub-type of the disease)
Sub-types of the disease and corresponding sub-sets of SOP/Care Plans is depicted below.
Alternative SOP/Care Plans Corresponding to Variations in Patient Profile and Disease Pattern (Image)
Expressing Variations As Alternative Segments
When the variation in case type and their care is slight there is no necessity to write separate SOP/Care Plans. Instead the difference in the care is expressed as alternatives in identified segments in the document.
Expressing Variations as Separate Documents
When the variation in the case type and its care is distinct then separate SOP/Care Plans should be prpared. For example, Bronchial Asthma is categorized based on variation in acuity of onset into Acute exacerbation and Chronic (long term) presentations. The two categories are very different in the approach to treatment. As such, there is no value in having a SOP/Care Plan for Bronchial Asthma per se. However, separate SOP/Care Plans have to be designed and written for the two categories with the common parts shared. Separate SOP/Care Plans are also needed for care of Bronchial Asthma in children.
Each of the categories (acute or chronic) has further sub-types based on severity. The differences of their care is mainly in the mode of treatment and intensity of monitoring. As such this variation in care of the disease sub-types is written as alternative segments/paragraphs (with headings) as shown below:
SOP for Varieties of Bronchial Asthma (Image)
