
- – First Published: July 21, 2014
- – Latest Revision: January 12, 2024
This article hopes to differentiate various information systems used in the field of health and healthcare. However, the main focus would be on the Hospital Information Systems.
OVERVIEW
It is common to think of information systems as the means to manage information or data. Yet, when used in a service like healthcare, the system should be considered as the use of computers as the means to facilitate the delivery of the service. Healthcare is a business activity consisting of various types of transactions (procedures).
The computerized system is made up of hardware and software to acquire, store, transmit, analyze and present information. The capability of information technology is leveraged to facilitate service delivery by relying on the ability of the computer to:
- provide information as an input when a task is to be performed,
- retain data produced as an outcome of the performance of the task,
- enable automation by transferring information to and from machines,
- provide information on the progress of operations (transactions, tasks) ,
- enable the sharing of data and
- enhancing and enabling communications.
Therefore, information systems are not just concerned with enabling the recording of information, but its use encompass the greater function of facilitating the delivery of services at operations level as well as its use later for strategic management and research .
Disambiguation of Terms
Health information management systems
A distinction must be made between health and healthcare. According to the World Health Organization (WHO), health is a state of complete physical, mental and social well-being and not merely the absence of disease or infirmity. Hence, health information is a generic term referring to anything at all to do with health. Since this involves a big amount of information, they have to be managed somehow. So, the systems that manage information concerning health are termed as health information management systems. It is a generic term, is always plural and the words are not capitalized. The scope encompasses many areas served by different systems. the acronym HIMS is invalid because it does not refer to a system for a specific purpose. However, the acronym HIMSS is valid because refers to the proper name of a society for the study of health information systems.
Healthcare is a service provided by an individual, a team of people or an organization. The term ‘care’ is used instead of the term ‘service delivery’.
Management refers to the job of planning, leading, and controlling the activities of an organization be it for manufacturing or service delivery. If the activity is confined to running the organization, it is termed as operations management, an activity led by an operations manager (chief executive officer or chief operations manager). The system used by the manager can then be called the Management Information System of the organization.
Health Management Information System of the Government (HMIS)
“Health management” refers to a wide range of efforts to promote, propagate, and manage issues relating to health. The two words should be taken together because only then it refers to the strategic management of health carried out by a large team of people. Factors contributing to people’s health include good nutrition, food safety, clean water, clean environment and a lifestyle conducive for health, not just the control of diseases. This broad range of activities is a societal responsibility usually taken up by governments. So, the system for it would be Health Management Information System.
Health management as a service, is usually taken up by the ministry or department within the government. The ministry of health being an arm of the government is responsible for managing all aspects the health of its citizens through of efforts at promoting health and the prevention, detection, control of diseases, regulation of healthcare services and provision of services to the sick. The ministry or department will then have within its organization an information system that facilitates the function of health management that would be called Health Management Information System (HMIS).
The system need not be completely computerized, but a computerized system would consist of applications that would facilitate the promotional, preventive, early detection (screening of disease) and treatment of diseases. It should enable the monitoring of disease incidence and prevalence so that it can help in the control of diseases (epidemiology). In addition, it should support the regulatory and supervisory functions of the government. As health is dependent on many factors, the system should enable coordination with other ministries.
The management of health relies mainly on strategic management approaches (forecasting, planning, budgeting, funding and control), Hence, information regarding the status, trends, and future needs of health and healthcare are required. Often, this information is derived from operational data obtained from healthcare services and all operations that affect health in one way or another. Another way of gaining information is through surveys and research. The information obtained is then gathered, stored, analyzed, and interpreted at a central office.
Healthcare Information Systems
‘Healthcare’ is the delivery of services concerned with health. It covers a broad area distinguished by aims that include:
- keeping persons healthy
- prevention of diseases
- the care of people when they become sick
The term used for the provision of service is ‘care’ and the industry is called ‘healthcare’. Hence, workers in the industry are known as ‘care providers’, healthcare workers’ or ‘healthcare professionals’. Non-professional persons giving care are often called care givers or carers.
Healthcare information systems is a generic term referring to a set of systems for the entire healthcare services encompassing patient care as well as services for the early detection of disease, prevention of health problems and promotion of wellness, at any location. The scope of healthcare is very wide. Basically, the systems are designed for two main divisions of healthcare i.e.,
- Wellness services information systems,
- Systems to facilitate the care of people when they become sick.
The two types of systems vary in content and design because of the difference in objectives and methods.
Services are provided by organizations. As such, systems are designed to cater for the type of services they provide. The scope can be confined to wellness-care or patient care or a mix of both. Because healthcare is a service, the healthcare information system facilitates operations or transactions (business of service provision). The information system (applications, databases and network) catering to each type of healthcare service is built around functions, policies and procedures (business rules) used to operate that service. Therefore, the system is said to be operational or transactional in nature.
Wellness services information system.
The service for the promotion of health, disease prevention and early detection of diseases of an individual can be called wellness care or service. The system is provided at a wide variety of outlets and by different service providers.
The system that supports it the wellness services information system.
- promotion of health
- primary prevention of disease (stopping the occurrence of diseases)
- early detection of diseases (screening)
Much of the objectives of health promotion are achieved through self-care or influencing people to practice a healthy lifestyle. Primary prevention relies on avoiding causes and building immunity. Good health deters disease. Early detection is achieved mainly through identification of risks, awareness of early symptoms or signs and health screening.
Information systems to facilitate the care of people when they become sick
The provision of services to people who are sick is termed as ‘patient care’. Often, it is also called ‘curative medicine’. The latter term is incorrect, since cure is not the aim in all cases. Other aims are the alleviation and mitigation of the effects of the disease. The generic term for such systems is ‘patient care information systems’.
Information systems to facilitate the delivery of patient care services are designed according to the type of facilities distinguished by the level of complexity of services it provides (primary, secondary, tertiary). Hence, we have Hospital Information Systems (HIS), Clinic Information Systems, Daycare Information Systems and Hospice Information systems etc. However, despite this differentiation into levels, the care of the sick (attending to the effects of disease) has the following basic functions:
- Diagnosis (identification of the health problem)
- Treatment (therapy, review of outcome and improvement)
- Rehabilitation
- Prevention
- secondary prevention (limiting the effects)
- tertiary prevention (regaining lost functions or improving it)
The information accumulated from these efforts are called the Medical Record.
Although the patient care information systems are built according to a generic pattern, each hospital, clinic or unit have to modify it to suit its peculiar needs.
Applications, the hardware and the network make up a system. Systems are built for facilities whereas applications are designed for functions. The various systems that serve healthcare services and functions are shown below.

Lifetime Health Records (Electronic Health Record – EHR)
The need for the care of an individual’s health is for a lifetime. Indeed, it begins at the time of conception, continues as the child grows up, experiences life as an adult and later in old age. The care includes efforts at the achievement of good health and the prevention, early detection plus treatment of disease.
The efforts occur at different sessions and are provided at different outlets. Therefore, ensuring consistency and persistence i.e., ‘the continuity of care’ is of paramount importance. This is achieved through the retention and sharing of information. Efforts are made to make available all information on a person’s health in an accessible location. The information regarding activities at achieving wellness can be termed as wellness health record and that for interventions when he or she happens to be sick can be termed as the medical record. Both types of information when compiled is what is termed as Electronic Health Record. The better name would be the Lifetime Health Record.
A patient’s entire medical record is a detailed record of events over a time period (the vertical health record). The degree of detail inherent in the EMR is necessary for the immediate care of the patient as well as a historical record for legal purposes. Trying to keep such an immense record for an entire population would require a lot of storage space. Since patient care is provided at a single or a cluster of facilities, keeping the Medical Record (EMR) is the legal responsibility of the management of those facilities, not that of a centralized body. On the other hand, the Lifetime Health Record should retain sufficient information to serve the need for continuity of care, which is a shared effort. It is a system for the sharing of information. Therefore, the Lifetime Health Record need to be made up of only summaries containing essential information. As a result, the volume of data is much more manageable. The summaries can take the form of documents which is much easier to store. Indeed, for clinicians, documents are much easier to read and understand as compared to structured data.
Summaries are reports derived from the database. To produce it, the extra effort required is the definition of what data need to go into them and the task of data extraction from the database of each participating facility. The role of the Medical Record Summary is as depicted below:

Facilities that provide wellness services (general practice, family practice, health clubs, health checks and screening facilities) should all contribute to the Lifetime Health Record.

The content of the Lifetime Health Record as contributed by the wellness services as well as the patient care services is as shown below:

The centralized nature of the Lifetime Health Record requires the use of a web-based application and the internet. It also presupposes that records at the primary source are electronic. Trying to get facilities to create summaries from paper records and submit them manually is an inconsiderate and impossible endeavor.

Administrative and Managerial Aspects
Like any other services the healthcare has to be properly managed to ensure viability, reliability and acceptability. Management has two tiers i.e.,
- Operations management
- Strategic management
The subject of systems for both administrative and managerial functions will be discussed later.
Patient care information systems: Hospital and Clinic Information Systems
People who are sick are called patients and their care is best termed as patient care. Hence, the generic term for the information systems applied to the service is patient care information systems. Since many activities are involved in patient care, with each activity being run on distinct set of policies and procedures, the patient care information system is made up many transactional information systems designed to facilitate each function. The patient care information system itself is designed to be an operational system that facilitates the work of care providers. While it has clinical data (from the Clinical Information System) at its core, it receives data from other systems. Therefore, it is best that it has a database that contains pertinent data replicated from other component systems.
Scale and Scope of the Patient care information system
Information systems to facilitate the delivery of healthcare services are developed for the type of facilities distinguished by the level of services and type of patients it provides. Hence, the generic term patient care information systems, when applied to these particular institutions, has been named as Hospital Information Systems (HIS), Clinic information systems, Daycare Information Systems and Hospice Information systems etc. The Hospital Information System is the most comprehensive and complex of all such systems. Knowing how it works will help in the understanding of less complex systems. Therefore, the Hospital Information System (HIS). is discussed in a bit more detail here.
The system, as described here, is also applicable to a free-standing general or specialty outpatient clinic.
HOSPITAL INFORMATION SYSTEM (HIS)
An information system that facilitates the activities of a hospital takes into consideration:
- the functions of a health care facility
- the capability of information technology
The information management system complements the other components of the very complex organizational structure and operations of a hospital. It acts as an integrator of all these components by enabling the collection, storage and sharing of information. The scope, content and structure of the Hospital Information System (HIS) serve many different functions. It contains a set of sub-systems and applications (often referred to as modules) that utilizes information-communications technology and computerization optimally to facilitate the delivery of services of the hospital.
In general, information systems of a healthcare facility facilitate two main group of activities, functions and services i.e.:
- The core business of providing healthcare to its clients
- Managing the hospital as a business entity, a provider of hospitality services and a physical facility
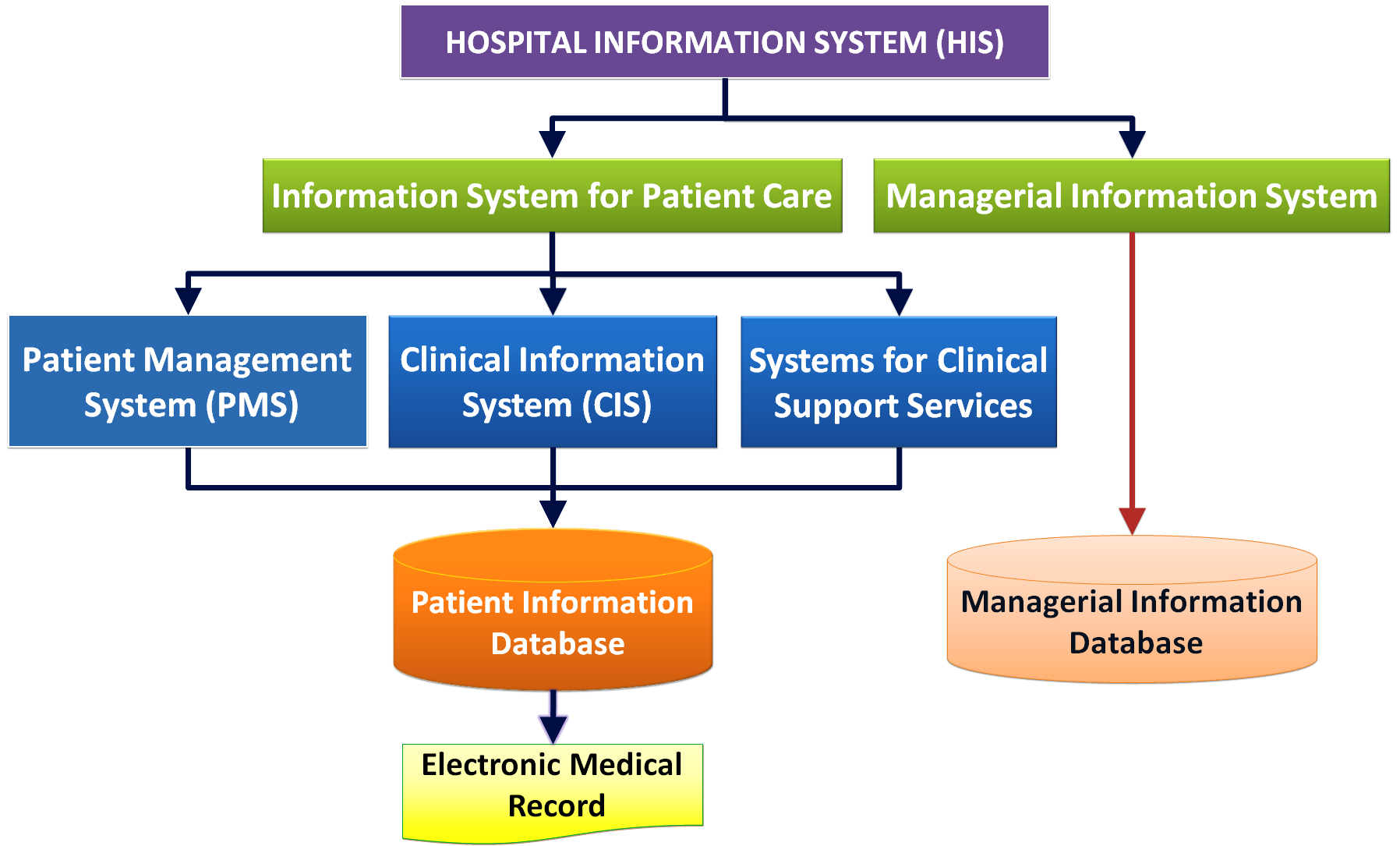
The Hospital Information System (HIS) is focused primarily on the Operations Management of the hospital. However, data available from the system may be collated, analyzed and used for strategic management including research. The HIS is envisaged as consisting of two broad systems i.e.
- Patient care information system
- Managerial information system
Main Divisions of HIS

The division into these two broad categories is conceptual. The information system that supports administrative, human resource, facility and hospitality management activities are placed arbitrarily under the managerial information system. This article and others in this website deals mainly with the Information systems for patient care function, i.e. the core business activity of a hospital.
Contributions to Other Health information systems
The Hospital Information System should be capable of sharing patient data with other health care institutions so as to enable continuity of care via the health information exchange or data warehouse or other means. It is expected to contribute to the national health database (in Malaysia: The National Health-Management Information System) by supplying information for health promotion, disease prevention and early detection efforts as well as for planning, resource allocation, epidemiology, case-mix calculations etc. at district, state and national level. It should also provide information to systems belonging to third party institutions e.g. external agencies like the Drug Safety Council, Registration Department, Road Safety Council, the Police, insurance companies and many others.
The Capability of Information Technology
A computerized information system opens many possibilities in data management. A major advantage is the storage of data in a database from which relevant data can be extracted and manipulated to create views and reports for specific purposes. These capabilities are depicted in the diagram below and will be explained further:

The capability of information systems is made possible by software and hardware hardware. The software consists of:
- System software
- Operating system for clients
- Operating system for servers
- Application programs
- Hardware
- Clients
- Servers
- Network
- cables
- wireless transmission
- switches and ports

HOSPITAL INFORMATION SYSTEM : CHARACTERISTICS
A Hospital Information System (HIS) can be designed and built in-house from the outset or purchased. Either way, the suite of applications software and databases need to be assessed or appraised to determine suitability for use before being made available to intended users. Systems purchased off the shelf, need to be customized to suit the hospital’s services, policies, procedures and equipment. On the other hand, some compromises in the existing processes may be required in order to align them with the requirements of computerization and use of information technology.
The data need to be stored in a properly designed database. The data structure is formulated by defining entities, relationships and naming of data elements and possible values attributed to each data element. This is achieved through the activity of Business Process Re-engineering, Customization and Database Design. An important aspect is the use of standard naming conventions peculiar to the hospital such as that for services, locations, care provider categories, visits, encounters and events. These static data elements are made available in reference tables. For variable data, universally accepted standard nomenclature such as Snomed CT, LOINC, ICD 10 Classification of Diagnosis would facilitate data sharing and data analysis.
At implementation, User Acceptance Testing should be thorough; initially on a Development/Build version of the system in a simulated Operations environment, and subsequently on the actual Operations/Production Version. After implementation the system has to be appraised continuously and improved upon if necessary.
Where legacy systems are retained they should be aligned with the structure and arrangement of the new HIS. A difficult issue is data migration. Success depends on ensuring technical compatibility as well as semantic consistency between the new database with the old data such that the data can be migrated into the new database and is accessible through the new applications. Data migration is discussed in a separate section.
Some devices and instruments may need to be replaced or new ones added to enable interfacing. There will be definite changes in the way data is collected because this needs to match with the data structure, collection and presentation used by the system.
SYSTEM INTEGRATION
The Hospital information system is not one single system but comprise of a set of systems. For ease of description, it is considered as consisting of modules consisting of the main application that facilitates the clinical function and other separate applications that support the clinical function. Hence , the HIS is a set of distributed systems with the Clinical Information System (CIS) at its center.
It is crucial that the Hospital Information System is fully integrated so as to function seamlessly across modules. Integration refers to the interaction between applications software with each other and with the hardware, enabling one to work with another for a desired purpose. Poor integration often makes it necessary for the user to go through extra steps to complete a task and also slows down the system response time. A substantial part of integration is the interfacing of information system computers with computers of peripheral hardware (machines, measuring apparatus etc.) enabling them to engage in transfer and retrieval of data or instructions. Integration needs to be addressed at the stage of HIS design as well as implementation.
It would be desirable to design or procure a HIS that have been fully integrated from the start and where the modules and sub-systems are proven to interact smoothly with acceptable response time and ease of use. Trying to integrate disparate applications software with different data structure and using different operation systems at the time of implementation would be an unenviable task. Integration usually involves two or more parties. Issues that can pose a stumbling block to speedy and successful implementation are sharing out of responsibilities, agreeing on a schedule and apportioning costs.
Another important consideration is the coordination between services and units within the hospital so that the each module takes into consideration differences in their policies and procedures. It would be desirable for these policies and procedures to be made complementary, uniform and standardized. Minor variations can be allowed.
ENABLING AND ENHANCING COMMUNICATIONS
Communications between care providers is of paramount importance. Various approaches and means can be used to facilitate and enhance communications. The main method is through the sharing of information. This is achieved by is placing data generated by each care provider in a common database and then making them available to others through views and displays tailored to the needs of various categories of users. Instructions, orders and reminders can be placed in the individual user’s in-box within an in-built e-mailing system. Messages can be relayed from the information system to users via both internal and external communications systems and devices such as computers (in-boxes, e-mails via intranet and internet), electronic white boards and mobile phones. Communications with patients can be through the same means, interactive kiosks and through web portals
INFORMATION SYSTEM FOR PATIENT CARE
The Hospital information System (HIS) can be broadly divided into two halves:
- The systems for the patient care function
- The managerial information systems
The clinical and other functions relating to the care of a patient is facilitated by a set of systems which can be given a generic name of Information Systems for the patient care function. The term Patient Care Information System is attractive and acceptable but, unfortunately, is used only by small number of advocates. This term will be used in all subsequent discussions here because having this extra category level as the parent, with the Clinical Information System (CIS) considered as a child, clarifies the nomenclature. The term Clinical Information System is not used to mean the whole information systems for patient care. Instead, the name CIS is confined to the system that facilitates or supports direct patient care functions (by clinicians). The other half of the system is the information systems for Clinical support services which are made up of several modules.
Conceptual Division of Systems for Patient Care

The term is ‘EMR/EHR Systems‘ is commonly used. This term is a misnomer and should not be used at all because information systems are useful only if they facilitate work rather than just “the creation, storage, and organization of electronic medical records” as understood by some.
OBJECTIVES & FUNCTIONS OF PATIENT CARE INFORMATION SYSTEM
Being a system for facilitating operations, these set of sub-systems and applications are expected to utilize computerization and information technology optimally to realize desired objectives in the following areas:
- Productivity
- Effectiveness
- Appropriateness
- Efficiency
- Quality
- Safety
- Privacy and confidentiality of information
To achieve the above objectives, the computerized information system is required to provide the following functions:
- Guide and enable the performance of Patient Care Processes
- Facilitate communication between care providers through sharing of information
- Enable automation of work processes through links within it, integration with other components of the hospital information system and interfacing with other computers, machines, printers and scanners
- Provide clinical decision support at point of care
- Gather, store and make available vital clinical information (individual and aggregated) for primary and secondary use
- Maintain a permanent record of events and all activities of patient care (as the Electronic Medical Record and other documents based on medico-legal requirements)
Any system being designed, proposed or implemented must possess characteristics that would fulfill all the above objectives and functions; both in its content and the methods used.
SCOPE, CONTENT & RELATIONSHIPS OF PATIENT CARE INFORMATION SYSTEM
The Patient Care Information System consists of:
- Patient/Client Management (Administration) Information System
- Clinical Information System (CIS)
- CIS for various specialties
- Clinical Documentation
- Clinical Decision Support
- Centralized Continuous Monitoring System
- Electronic Medical Record
- Clinical Support Systems
- Laboratory Information System
- Blood Banking Information System
- Radiology Information System
- Pharmacy Information System
- Food and Beverage Supply System
- Operation Theatre / Suite Information System
- Sterilization and Sterile Inventory & Supplies System
- Other support systems
- Bridging or intermediary systems
- Order entry – Result reporting system (CPOE)
- Patient information database management system
- Applications that support Clinical Governance
- Decision support application for clinical managers
- Quality and productivity management application
- Infection Prevention and Control Application
- Clinical data extraction and reporting application
- Means of supplying data to external organizations
The relationships of the systems are as depicted the chart below:
Healthcare Information System
All the above systems are used by health care personnel to care for patients. Care is here defined as all work activities to deliver services to patients in response to their needs.
Clinical Information System
The Clinical Information System (CIS) facilitates direct patient care i.e. activities of care providers i.e. mainly doctors and nurses but also includes Dietitians, Therapists, Clinical psychologists, Clinical pharmacists, Clinical Microbiologists, Interventional Radiologists, Endoscopists, Optometrists, Audiologists and many others. A good CIS provides assistance and guidance for clinicians to perform their work besides capturing pertinent data that is generated.
The CIS contains application modules (however named) that enable the following:
- Planning of care (use of Care Plans)
- Provision of clinical decision support
- Clinical data documentation or capture (Data entry)
- Quality Control
- Data Storage
- Data Retrieval and Display

A detailed discussion of the Clinical Information System is provided in a separate article.
Clinical support systems
Clinical support refers to services that:
- perform tests
- provide supplies
Direct care providers request for these services through the Order entry functionality. Test results are submitted to the database from where they are made available. Supplies like drugs, blood products, sterile supplies and food are delivered to persons/units requesting them. Their delivery and receipt are recorded in the database.
System for Clinical Support Services

INTEGRATION OF THE COMPONENTS PATIENT CARE INFORMATION SYSTEM
Integration within the Patient Care Information System is essential. The smooth running of this system are dependent on proper linkages between sub-systems/modules within it. It is desirable that they are already fully integrated at the time of procurement.
KEY BRIDGING APPLICATIONS
The main patient care applications software i.e. the Clinical Information System and the various Clinical Support Systems are built around key bridging (intermediary) components i.e.
- Patient Administration/Management System (Registration, Scheduling, Resource allocation)
- Order-Entry Result Reporting Application (CPOE)
- Database Management System (DBMS)
- Electronic Medical Record
- A common user-system interface (front end screen, GUI)
These applications are thought of and designed first and then amended as each clinical and clinical-support application is designed. Additional applications software are configured to be compatible with these key bridging (intermediary) applications.
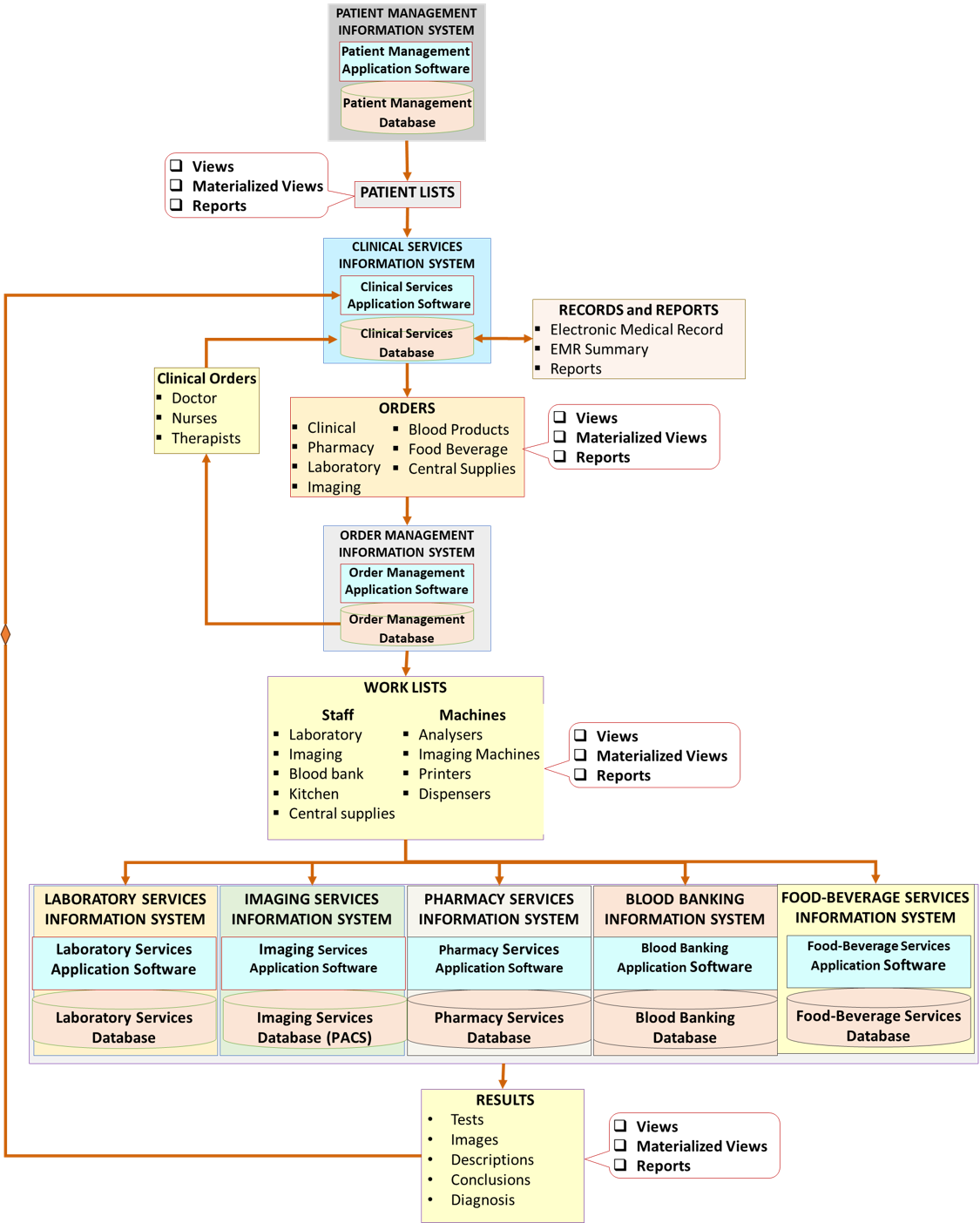
The relationships between the five key applications or functionalities of the patient care information system is shown in the chart below:

Each of these applications is discussed further below.
Role of Patient Administration/Management System (PMS)
The Patient Administration/Management System (PMS) supplies identification, demographic and other static data such as payment class to the Patient Registration Database (Patient Master Index). Other systems derive these data from the database thus ensuring that they are standardized and making it unnecessary for them to be obtained repeatedly.
The most important role is in attaching identity to patients, samples, equipment, locations and services. Confirmation of identity is necessary before records are accessed, data is entered, tests are done and treatment is given. One method is to use bar-coded labels on specimens and wrist-bands combined with the use of scanners.
Components of Patient/Client Management/Administration System

Contribution of Identification and Demographic Data to Other Sub-Systems of the Patient Care Information System
Data acquired through the Patient Management Information System is shared will almost all other sub-systems. Even so, although much data is acquired regarding a patient, only a sub-set of the data may be required by the different different systems. Identification data is of paramount importance for all sub-systems.
Creation of Patient Lists
The Clinical Information System will probably require all identification, demographic data and resource management data. This data is provided by creating patient lists for each service unit (inpatient, outpatient, emergency, intensive care etc.). The list is a view created by querying the current patient in the registry (Patient Master Index) in real-time. Because patients are continuously being admitted or discharged the list must be continuously updated. Therefore, there is a continuous interaction between the Clinical Information System and the Patient Administration/Management System (PMS)
Role of Order Entry-Result Reporting (Order Management) Application
The Order Entry application acts as a means of communications between care providers and the tool for planning, initiation and execution of processes or tasks. It enables transactions started in one module to go across to another module and be executed. It is essential that an order is made on the correct patient or the sample from the correct patient. Orders are made on patients listed in the Patient List of service units. Orders should not be made on patients not incepted (registered) into a service. The exception is for future orders which have a tentative status until the patient is registered.
Labels printed with identification data can be attached to samples so that the patient identity is known, and results can be placed in his/her record in the database.
The Order Entry -Result Reporting Function

Order entry is the primary mechanism for executing care plans. Each plan can be made up of sets of pertinent orders indicated for a session or indication.
Worklists
Worklists are created from orders made on patients of the service unit. The units responsible for carrying out the orders will have their own worklists. These units, for example the Pharmacy, Laboratory and the Imaging Systems, will require identification data, data on age and gender and session and location data.
The principal entity in the Laboratory System is the sample. The Laboratory System database would be a collection of data about samples. Identification and demographic data are descriptors that identify the sample. They are supplied to the system when the order is made and appear on the worklists for work desks or machines. The sample is matched with the item on the worklist by scanning the (bar-code) label on the container. There is no necessity to query the Patient Registration Database. Therefore, users must ensure that information on the patient or sample is accurate when the order is made.

Similarly, in the imaging application, the principal entity is the image (individually or as a set). The Imaging System database would be a collection of data about images. Identification and demographic data are descriptors that identify the images. They are supplied to the system when the order is made and then transferred to worklists on work-desks and machines. The identity of the patient is confirmed by identifying the patient when he/she arrives either manually or by scanning the bar-code label on the wrist band.

The Clinical Information System as a Consolidation of Various Distributed Systems
The core function of patient care service is the clinical care of patients. As such the Clinical Care System is the principal system. It interacts with other sub-systems in different ways. As discussed earlier the interaction with the Patient Administration / Management System and the Order Mangement System is very intimate and need to be in real-time.
Interactions with clinical support systems is via the Order Mangement System and requires a near-real time latency. Data from the clinical support systems (status and results) are provided in the presentation layer as views, materialized views or reports. This function is called the Result Reporting function. While views are transient, materialized views and reports are incorporated into the Patient information Database and made available as part of the Medical record. The data is dynamic by being constantly updated or modified.

to be retained
Role of Patient Information Database
The ability to share data is essential for the success of an integrated HIS. The Patient Information Database enables data generated and submitted by each user to be stored and then shared with others through displays on the computer screen, or printed material (documents and labels). Accumulated data can be analyzed using various tools to create reports for clinical and managerial use.
The chart below depicts how of Information is shared through a common database

The data required for clinical patient care comes from multiple sources. The clinician must be able to access the relevant data easily without having to go through several individual applications. Pertinent data from other applications are replicated in timely manner and merged with clinical data gathered by clinicians. The database the created in this way is termed as an operational database.
The Patient Information Database contains all the information necessary for the clinical care of the patient not just data generated by clinicians. The Electronic Medical Record is derived by extracting data from this database. Also, it contains the essential data to be retained when the system is changed or upgraded such that it enables:
- Business continuity
- Continuity of care
- Preservation of a historical record for medico-legal purposes.
Secondary Use of Patient Data
The capability to analyze, interpret and make them available as reports to managers and external agencies (e.g. the Ministry of Health) should be in-built in any HIS. Otherwise a third party analysis and reporting system need to be procured. Its function would be to and keep them in a repository before distributing them to agencies involved in planning, budgeting, resource allocation and performance monitoring.
Reports are used by various users and managers of the institution or at higher management levels to:
- facilitate the business managerial functions and clinical governance within the hospital/health care facility
- provide data to external agencies (e.g. those within the Ministry of Health) for use at the community and national levels
Hospitals would require reports that are standard (routine, used on a regular basis) plus as and when required (ad hoc). Data from a group of patients can be extracted and manipulated, for purposes of managerial oversight, audit and research. At a higher level essentials reports that can be generated include those for determining current performance such as Key Performance Indicators (KPIs), the Health Management Information System Reports (HMIS), Information Documentation System Reports (IDS), Disease or Procedure Registry Reports and Quality Assurance reports.
Data can also be exported to other systems such as:
- Shared operations database(s) where patient data is made available to other institutions for purposes of patient care
- Data warehouse(s) where anonymized patient data is pooled and used for Management Information Systems (strategic management, financial management, Enterprise Resource Planning), Disease Prevention and Control, Public health, Epidemiology), and research.

Role of Medical Record
The traditional function of the paper-based Medical Record is to retain and make available historical data for use by current and future clinical users for continuity of care and to non-clinical users for various valid purposes. In a computerized environment, most of the functions of the paper record (i.e. the capture, storage, distribution and communication of data) is taken over by the Patient Information Database. During care, providers (clinical and non-clinical) submit, record and retrieve data to and from this database rather than directly into the Electronic Medical Record. Clinical information is presented as displays. However, it is still necessary to create and maintain a Medical Record of each patient, for:
- a display of the chronology of events for an understanding by care providers of care already given
- a chronological record of events for medico-legal and professional purposes.
Therefore, the content and arrangement of data in the clinical applications and database need to take into account of the legal and professional requirements of the Medical Record. Generation of the Electronic Medical Record is accomplished through a specially designed data extraction application using a query tool that defines its content and structure. It can then be printed if necessary or made available in various format. The EMR is discussed further in another article.
Role of Common User-System Interface (GUI)
Users of information systems input and retrieve via the presentation Logic / Layer of the system. It is important for the user-system interface, i.e. the front-end screen viewed by users to access applications and input/retrieve data, to be similar for all instances of use of the system. The interface is made to be intuitive and familiar by fixing positions, shapes and color scheme of the navigation menu and by standardizing the way they operate. It is best that the set of applications or views required by a user is made available to him/her, on log-in, by matching them with his/her role. The need to log-in and out of various applications should be minimized.

INTEGRATION WITH THE REST OF HIS
It is crucial that the Information System that the Patient Care Function is able to integrate with other systems of HIS. For the sake of choosing the best of the breed, it may be necessary to procure separate systems or modules from different vendors. Due consideration must be given to areas where Management Information Systems interact with the Information System for the Patient Care Function. Examples of such areas are Charging and Billing, Human Resource deployment, Bed allocation and Food-Beverage services. It is imperative that these are demonstrated to be capable of full integration with the rest of HIS.
Use of a common Patient Information Database and good data extraction-analysis tools will support the activities of incident reporting, clinical epidemiology, disease surveillance, quality management, utilization review, risk management and similar functions.
MANAGERIAL INFORMATION SYSTEM
FUNCTIONS OF OPERATIONS MANAGEMENT
The Operations Management Information System refer to the set of sub-systems and applications that assist managers in running the hospital as a:
- business entity
- provider of hospitality services
- physical facility
The term ‘managerial’ is generic and refers to a set of sub-systems useful for managers. It is used here because other terms such as Management / Operations / Business / Enterprise Resource Planning systems have their own usage.
COMPONENTS OF OPERATIONS MANAGEMENT SYSTEM
Systems that support the business operations include:
- General Administration Information System & Office Automation
- Charging, Billing and Receipt of Payment (Accounting) System
- Human Resources Management System
- Finance and Budgetary Systems
- Consumables Purchasing and Inventory System
Systems for facilitating the hospitality services of a hospital include:
- Bed management
- Food-Beverage Order-Supply System
Systems for management of the hospital as a physical facility include:
- Facility Engineering Systems
- Equipment and Machinery Maintenance and Inventory System
- Environmental Safety, Housekeeping, Cleansing and Waste Management
Managerial Decision Support Systems (DSS) can be very helpful and include:
- Business Management Decision Support
- Clinical Governance Decision Support
The DSS to be implemented can be variable complexity. It can range from simple statistical tools to business intelligence software. Large organizations may also want to create a Data Warehouse and use Enterprise Resource Planning software.
The components making up the Managerial Information System is wide-ranging and complex. They are not within the scope of this discussion (at this point) but mentioned here for completion. However certain components that integrate or interface with the Information System for Patient Care Function will be discussed.
Management Information Systems
Information systems for the managerial functions belong to two categories has two tiers i.e.,
- Operations management Information System
- Strategic Management Information System
Operations Management Information Systems
Operational systems management information systems facilitates the day to day running of the business of healthcare. The administrative and managerial approaches are quite similar in all the systems involved in healthcare. However in terms of objectives and methods, patient care and wellness services follow their own paradigms. In modern patient care practice, clinical care providers includes doctors, nurses, allied health personnel and other professionals adopt a universally accepted principles, concepts and methods. Patient care is usually provided in facilities that includes hospitals, clinics and daycare units. Wellness services is concerned with the general population who are well. Services are provided at the community (usually by government agencies) and at service facilities. The operational managerial function is facilitated by a separate information system. It often called the Enterprise Resource Planning System which is perhaps a misnomer, because it is not only about resources nor is it confined to planning. Rather, it concerns itself with all aspects of management. It is designed for a facility (like a hospital) rather than an enterprise. The planning involved is the planning of operations rather than strategic.

Strategic Management Information Systems
Strategic management is concerned with how to ensure that business survives, continue to improve and possibly expand. It uses research and strategic tactics. Data accumulated during operations (from the operational management system database) is analyzed to determine the current status and trends (achievements vs failures). This is compared with status and trends of similar organizations. Opportunities arising from new knowledge or technology are appraised and used to make corrections and plan improvements. This is an area where an analytical database or a data warehouse would be useful. The functions of strategic management include:
- Business Development Planning
- Human Resource Planning
- Product/Service Quality Planning
- Product Development Research and Planning
- Finance & Budgetary Planning
- Asset & Material Resource Planning
- Technology Adoption Research & Planning
- Marketing Research
- Risk Management Planning

Both types of management information system will not be discussed in detail on this site.
I would appreciate if you can leave any comment or suggestion in the box below or write to me at drdollah@gmail.com

Leave a Comment